

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ovarian cancer is the eighth most common malignancy in women worldwide with a mortality rate of over 140,000 deaths per year.1 Borderline ovarian tumors (BOT) are recognized as a vague entity of ovarian tumors between benign and malignant tumors. BOTs are typically detected 20 years earlier than invasive ovarian carcinoma.2
The annual incidence of BOT is 1.5-2.5 per 100,000 and approximately 3,000 cases of BOT are diagnosed each year in the United States.3 Since the 1970s BOT has become more common among white women of reproductive age. BOT is classified into five categories among which the most common types are serous and mucinous. For the serous type, 70% of cases are stage I with a survival rate of almost 100% and 30% are advanced stage with a survival rate of 95.3%. For the mucinous type, 82% of cases are stage I with a survival rate of 99-100% and 18% are advanced stages with a survival rate of 50%.4 Some studies have reported that the recurrence rate for BOT ranges from 8% to 32%.5
Hereditary ovarian cancer represents approximately 10% of all epithelial ovarian cancers.6,7 The two most common hereditary cancer syndromes with regard to ovarian cancer are hereditary breast and ovarian cancer (HBOC) and Lynch syndrome, also known as hereditary nonpolyposis colorectal cancer (HNPCC). HBOC accounts for approximately 90% of cases, and the remaining 10% are attributable to Lynch syndrome. The frequency of breast cancer 1, early onset (BRCA1) or breast cancer 2, early onset (BRCA2) mutations in the general population is estimated to be between 1 in 300 and 1 in 800.8 BRCA1/2 are located on chromosomes 17q21 (22 exons, 80 kb DNA) and 13q12-13 (26 exons, 70 kb DNA)9,10 respectively. The ovarian cancer risk among patients with Lynch syndrome is 12%.11 And Lynch syndrome is increased endometrial cancer by 42% to 54%. However, someone with no family history of Lynch syndrome affected endometrial cancer was reported.12 The most two affected genes are mutL homolog 1 (MLH1; 40-45% of cases), mutS homolog 2 (MSH2; 40-45%).13
Some studies on the genetic background of BOT were recently reported. A small proportion of BOT patients are known to have a somatic mutation.14 Another genetic test for BOT showed the possibility of an additional treatment based on gene sequencing results.15 However, little is known about germ line mutations in BOT, therefore in this study we assessed the hereditary risk of BOT based on immunohistochemistry (IHC) analysis.
Materials and Methods
Thirty-four women with BOT and available tumor blocks were identified among patients being treated in department of Obstetrics and Gynecology, Samsung Chang-won Hospital since 2003 and 2013.
After Institutional Review Board (IRB) approval (IRB No: 2012-SCMC-028-00), family history, clinical characteristics were collected through medical charts review. IHC was performed on all tumor specimens to determine the protein expression of BRCA1, BRCA2, MSH2, and MLH1. For IHC analysis monoclonal antibodies against MSH2 (Novocastra Laboratories Ltd., Newcastle upon Tyne, UK), MLH1 (Novocastra Laboratories Ltd., Newcastle upon Tyne, UK), BRCA1 (Abcam Ltd., Cambridge, UK), and BRCA2 (Abcam Ltd., Cambridge, UK) were used. Immunostaining was performed using the Bond-Max immunostainer (Leica Biosystems Newcastle Ltd., Newcastle Upon Tyne, UK) according to the manufacturer's instructions. Normal staining patterns for MSH2, MLH1, BRCA1, and BRCA2 were nuclear staining. Loss of expression in cancer cells was demonstrated by the total absence of nuclear staining in the tumor. Adjacent normal stroma or infiltrating lymphocytes served as an internal positive control for each case.
All cases were evaluated by dedicated two gynecologic pathologists two times. Staining was scored based on the intensity and proportion as follows: negative (or 0 and 1): intensity undetectable or minimal, proportion < 5%; 1+: intensity mild, proportion 5-30%; positive (or 2+): intensity moderate to marked, proportion 30-100% (Fig. 1). Two cases were excluded from analysis, one had only pathologic slides and the other lacked BRCA1 IHC analysis.
Finally, 32 cases were analyzed for the following demographic characteristics: age, menopause, parity, CA-125 level, and progression-free survival (PFS). We used chi-square or Fisher exact test for categorical variables. A P value < 0.05 was considered statistically significant. Statistical analyses were performed with SPSS software (version 12.0; SPSS Inc., Chicago, IL, USA).
Results
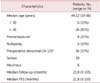
Among the 34 cases with available tumors, two cases were excluded due to incomplete data. The demographic characteristics for the 32 patients are listed in Table 1. The median age at diagnosis was 44 years (range, 19 to 86 years), and 81% of cases were older than 30 years. Eight women (25%) were premenopausal and six (19%) were nulliparous. Among 31 cases, 16 (57%) had abnormal cancer antigen 125 (CA-125; level > 35 U/mL) before surgery. Among patients with an abnormal CA-125 level the pathologic distribution was 63% serous type and 37% mucinous type. Analysis of family history of the patients showed no family cancer history in their medical charts. The median follow up period was 21.8 months (range 0-105) and no cases showed recurrence. The median PFS was 21.8 months (range 0-105).
Regarding histology, 14 patients (44%) were serous type, and 18 (56%) were mucinous type (Table 2).
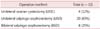
Patients were classified into three groups by operation method: unilateral ovarian cystectomy (UOC), unilateral salpingo-oophorectomy (USO), and bilateral salpingo-oophorectomy (BSO) including total hysterectomy. All 32 patients underwent surgery, and the number of UOC, USO, and BSO procedures was 4 (12%), 20 (63%), and 8 (25%) respectively (Table 3). UOC cases undertook re-staging operation later.
IHC analysis of four hereditary related genes was conducted on tumor blocks. None of the samples showed loss of expression, as indicated by negative IHC staining, but weak staining was found for MSH2 (n = 1, 3%) and BRCA2 (n = 6, 19%). The pathology of the patient with weak MSH2 staining was mucinous and that of the patients with weak BRCA2 staining was serous (n = 2) or mucinous (n = 3) (Table 4).
Interestingly, one patient with a serous borderline tumor was also diagnosed with a serous cystadenocarcinoma at the same time. Before the operation, her serum CA-125 was elevated (554.7 U/mL) and the computed tomography (CT) image indicated a malignant appearance for the right ovarian mass. The patient underwent BSO, total hysterectomy, pelvic lymph node dissection, total omentectomy, and an appendectomy for surgical staging. Based on surgical findings from frozen biopsy the left ovary looked normal but the right ovarian mass was malignant. The final pathologic finding was serous borderline tumor in the left ovary and serous cystadenocarcinoma in the right ovary. We obtained IHC data corresponding to both tumors, which showed the same result of weak BRCA2 staining and strong staining for the other markers for both tumors.
Discussion
There were 2,124 newly detected cases of ovarian cancer and the estimated mortality was 987 in Korea.16 Theory has been proposed regarding carcinogenesis of ovarian carcinoma designated type I and type II.17,18 Type I, or borderline, tumors are low-grade serous carcinoma, mucinous carcinoma, endometrioid carcinoma, malignant Brenner tumor, and clear cell carcinoma, whereas Type II tumors are high-grade serous carcinoma. These two types differ in their pathogenesis, molecular events, behavior, and prognosis, and it is rare for a low-grade serous carcinoma to change to a high-grade serous carcinoma.17,18 But hereditary background has not been fully studied so far.
Difficulties with ovarian carcinomas are hardness to diagnose early and cost to treat them.
Most ovarian carcinoma patients do not have specific symptoms and 16% are asymptomatic at the time of diagnosis.19 As a result, when they are diagnosed the stage tends to be more advanced. In addition, treatment costs for cancer are increasing.20 Early diagnosis of ovarian cancer is difficult, but very important. We do not know exactly what proportion of BOT represent suspicious ovarian carcinoma or a hereditary cancer risk, although it is believed to be small.
BOT are a transitional category between benign and malignant. The prognosis of BOTs is generally good,21 but they can recur or change cancer type. In one study, 28 women (17%) showed recurrence as either BOT (23 womens) or carcinoma (5 womens) after fertility-sparing surgery for BOT.22 In another study, the recurrence rate of serous BOT with non-invasive implants was 44% and the mortality was 25%.5 In some cases BOT is diagnosed concurrently with serous cystadenocarcinoma, as seen in our study.
The exact hereditary risk of cancer associated with BOT is unknown. There currently is no direct evidence that BOT is associated with hereditary ovarian tumor although several studies have evaluated the pathologic features of hereditary ovarian cancer.23 Among 11 studies of HBOC, one study reported a single mucinous borderline tumor among 13 cases of cancer associated with BRCA1 mutation.24 The pathologic features of Lynch syndrome patients indicate that more than 90% of the tumors are carcinomas, with borderline tumors representing only 4.1% of the epithelial cancers.25
Therefore, there is a possible association between HBOC or Lynch syndrome and BOT. Many studies of BOT are ongoing, but few are evaluating the hereditary risk. Our study reveals a potential hereditary risk of cancer among BOT patients and suggests that between 3% and 19% of patients may need genetic counseling and confirmative testing.
Our study is the first preliminary study of the hereditary risk of BOT using IHC. Our diagnosis was based on several clinical and IHC criteria. One previous study showed a strong correlation between BRCA1 IHC data and molecular events in ovarian cancer26 and another study showed the feasibility of IHC for detecting Lynch syndrome.27 For initial screening of Lynch syndrome the most commonly used test is IHC with 82.6% in endometrial tumor screening and 64.2% in colorectal tumor screening.28
A recent study involving whole exome analysis of low-grade serous ovarian carcinomas identified an average of only 10 somatic mutations per tumor in seven cases.29 Another study that examined the entire exome of serous BOTs for somatic genetic mutations showed similar results to low-grade serous carcinomas14. We should therefore consider hereditary risk, rather than somatic mutation.
There are studies for markers of ovarian tumor. Expression of p53 and Jab1 proteins is showed positive trend of ovarian cancer, but expression of p27 protein is related negative effect.30 In other hands, benign tumor, such as endometriosis, is associated Estrogen receptor gene polymorphisms.31
Our studies indicate the need for a large prospective stu dy of BOT. Further studies should evaluate the cost effectiveness and appropriate selection of candidates for genetic testing. We also recommend MLH1, MSH2, BRCA1, and BRCA2 IHC analysis during operative pathology for patients with ovarian masses, and cooperation and close follow-up with a pathologist.
In summary, our study is the first report of the risk of hereditary borderline ovarian cancer in gynecologic malignancy patients in Korea based on clinical and IHC criteria (MLH1, MSH2, BRCA1, and BRCA2 protein expression). We found that 3% and 19% of women with borderline ovarian cancer had relevant MSH2 and BRCA2 IHC data respectively, suggesting that a small proportion of patients might need genetic counseling and gene sequencing for hereditary risk evaluation. Identification of patients with borderline cancer through the acquisition of family history, IHC, and CA-125 data can prepare us for better consultation and might prevent the development of more advanced cancers.



 XML Download
XML Download