

 PDF
PDF Citation
Citation Print
Print



I. Introduction
Dentigerous cysts are usually related to impacted or unerupted teeth, are the second most common odontogenic cysts after radicular cysts, and account for approximately 24% of all epithelium lined jaw cysts1. They are more frequent in the second and third decades of life, with a male preference and the mandible being the most influenced region2. These cysts can lead to cortical bone expansion, swelling, and tooth mobility and displacement3. The radiographic image of a dentigerous cyst shows well-defined unilocular radiolucency, often with a sclerotic border, surrounding the crown of an unerupted tooth4. If these cysts are not treated, they can cause pathologic fractures, impaction of the permanent tooth, and bone deformities. The methods for treating dentigerous cysts usually consist of surgical techniques such as marsupialization and enucleation. Marsupialization can sustain the impacted tooth in the cystic cavity and encourage its eruption5. Marsupialization is particularly useful for dentigerous cysts with tooth displacement. Marsupialization can permit the eruption of a cyst associated with an impacted or unerupted tooth if enough space exists6.
We present a case report of a 7-year-old female patient with an unerupted mandibular left permanent second premolar associated with an infected dentigerous cyst that was treated with marsupialization. We performed the marsupialization technique accounting for the possibility of physiologic eruption of the permanent tooth related to the cyst without orthodontic follow-up or any other treatment.
The study approved by the İzmir Katip Çelebi University Ethical Committee (IRB no. 125), and informed consent was obtained.
II. Case Report
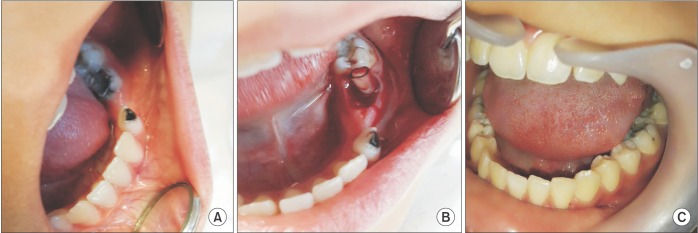
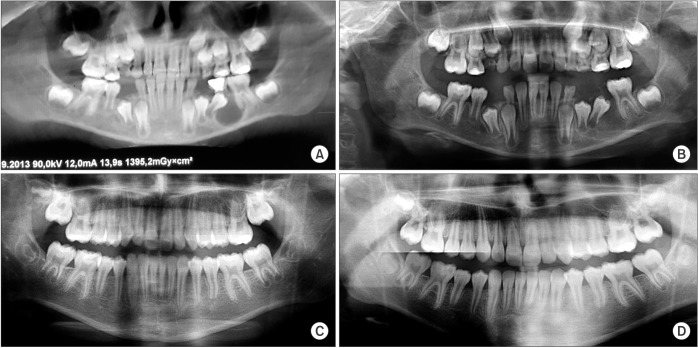
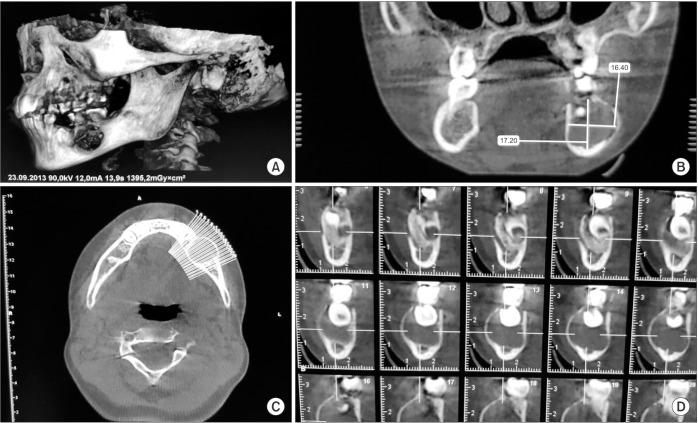
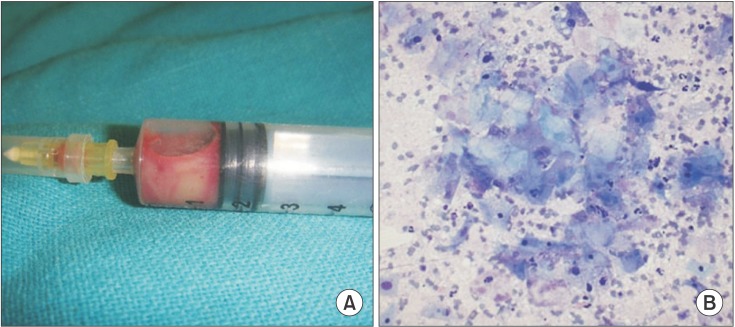
A 7-year-old female patient was referred to our clinic for treatment of a lesion in the lower left vestibule detected through routine panoramic radiography. Her past medical history and general physical examination were unremarkable, with no systemic problems and no report of pain or changed sensation. Physical examination revealed a mass, suggesting a hard submucosal lesion, in the lower left vestibule. (Fig. 1. A) Carious lesions were observed in the mandibular left second primary molar. A panoramic radiograph revealed a well-defined osteolytic lesion that measured 2.5 cm in diameter in proximity to the unerupted second premolar and displacing the tooth to the lower border of the mandible.(Fig. 2. A) A cone-beam computed tomography (CBCT) image was acquired because of the large size of the lesion.(Fig. 3. A) CBCT imaging revealed a well-defined lesion in the mandibular left region surrounding the crown of the unerupted second premolar. The apex of the tooth was still open.(Fig. 3. B-D) There were no signs of root resorption in the adjacent tooth. The swollen mass was aspirated and sent for biopsy of thick blood mixed mucoid material.(Fig. 4. A) The cytopathologic analysis of the aspirate revealed a mucoid material with clumps of benign epithelial cells and a large number of cyst macrophages.(Fig. 4. B) A temporary diagnosis of the inflammatory type of dentigerous cyst was made based on the aforementioned findings. Under local anesthesia, the patient was treated by extraction of the mandibular left second primary molar. A preventive approach was followed to preserve the developing mandibular left second premolar. Decompression of the cyst was performed using a silicone tube through the socket of the tooth extraction site over the lesion.(Fig. 1. B) The silicone tube was secured with sutures to the gingival tissue. The drain was maintained for 6 months and irrigated 3 times a day. The 9-month follow-up visit showed a reduction in radiographic radiolucency with spontaneous eruption of the tooth.(Fig. 2. B) There was further occlusal movement of the tooth and almost complete reduction of the radiolucency. A panoramic image showed almost complete ossification of the bony defect and further occlusal movement of the tooth as well as continuation of root formation. The clinical and radiographic evidence after 40 months showed that the second premolar had successfully erupted without orthodontic intervention or any other treatment.(Fig. 1. C, 2. C) The 46-month follow-up visit showed nearly complete root formation of the mandibular left second premolar.(Fig. 2. D and 5)
IV. Discussion
As with most odontogenic cysts, surgical methods such as marsupialization, decompression, and enucleation are used in treatment. Marsupialization procedures have been reported to be an effective treatment method, especially in pediatric patients, to prevent permanent damage to tooth buds in the treatment of large dentigerous cysts7. It is believed that new bone processing is stimulated because marsupialization decreases intracystic pressure. The disadvantage of marsupialization is the remaining pathologic tissue left in situ that cannot be verified without a thorough histologic examination. Even though the removed tissue can be presented for pathologic examination, there is a possibility of a more aggressive lesion present in the residual tissue such as ameloblastoma, squamous cell carcinoma, or intraosseous mucoepidermoid carcinoma8.
The treatment of a dentigerous cyst relies on the size and location of the cyst, patient age, and cyst proximity to vital structures. Marsupialization or decompression is indicated for pre-adolescents to protect the teeth and encourage the eruption of the dislocated tooth related to the cystic lesion. Marsupialization maintains the impacted tooth in the cystic cavity and supports its eruption by decreasing intracystic pressure through the creation of an accessory cavity9. Several instruments have been identified to reopen the area after marsupialization. Some authors have described the utilization of small-diameter silicone tubes of several lengths10. Instruments with an inner lumen are advantageous in that they do not need to be changed and are more hygienic in the cavity, eliminating the need for frequent visits to the clinic. This is especially important for pediatric patients, in whom washing out small food debris from the depth of the cavity and complying with the need for thrice-daily rinsing with an injector can be difficult11.
Serra e Silva et al.12 chose the marsupialization technique for a 10-year-old boy with a dentigerous cyst adjacent to his unerupted first premolars. The authors observed that, after three months, the radiographic radiolucency had decreased, and the premolar had started to erupt without any other treatment. After 30 months, the premolar had erupted successfully. In this case report, marsupialization was the treatment of choice instead of enucleation of the cystic lesion because the patient was young, the lesion occupied a large area of the mandible, and the cyst had caused displacement of the premolar.
Hayasaki et al.13 used the marsupialization technique in a 4-year, 2-month-old girl because of dentigerous cysts around her mandibular right second premolar. The authors extracted her primary mandibular right second molar and placed a removable appliance with a resin projection into the socket of the extracted tooth and the cystic cavity. The authors reported, however, that the appliance had to be extracted because it had not healed normally in postoperative follow-up14. In this case study, the marsupialization technique and a careful waiting period for the spontaneous eruption of the unerupted tooth, without orthodontic treatment, resulted in a successful outcome. A silicone tube was used to reduce the intracystic pressure and replaced monthly for 6 months postoperatively.
Park et al.14 reported that marsupialization is helpful for promoting the eruption of teeth related to dentigerous cysts, keratocystic odontogenic tumors, and unicystic ameloblastomas. Takagi and Koyama15 also reported that the orthodontic treatment of impacted teeth with mature roots has often been carried out after marsupialization of a large cyst. In the present case, the tooth erupted with only marsupialization without orthodontic treatment.
In conclusion, conservative surgical treatment methods can be the first option for treatment of dentigerous cysts in pre-adolescents to protect and encourage the eruption of permanent teeth. Marsupialization is an effective surgical technique, even for an infected cyst. Pre-adolescent patients and their parents must understand the importance of good oral hygiene for a successful treatment outcome.
 XML Download
XML Download