

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Tooth is a composite structure consisting of inorganic components including the calcium phosphate lineage and organic components such as collagen. Tooth minerals consist of five biological calcium phosphates: hydroxyapatite, tricalcium phosphate (TCP), octacalcium phosphate (OCP), amorphous calcium phosphate (ACP), and dicalcium phosphate dehydrate. Interacting reciprocally, these calcium phosphates are capable of remodeling the existing bone when grafted. The apatite existing within the bone tissue is known to be in the form of ceramics/high-polymer nano-composites.
Teeth and bones share many similarities. Teeth, cartilages, nerves, and maxillofacial bones all embryologically originated in the neural crest, sharing identical origin1-4. Clinicians support the intramembranous bone formation pathway when intraoral bone grafting is achieved5,6. The chemical compositions of teeth, especially dentin and bones, are very similar. Enamel consists of 96% inorganic substances and 4% water, whereas dentin has 65% inorganic substances, 35% organic substances, and water. Cementum is made up of 45-50% inorganic substances, 50-55% organic substances, and water. Finally, alveolar bone has 65% inorganic and 35% organic substances.
In organic parts, dentin and cementum include type I collagens and various growth factors such as bone morphogenic proteins (BMPs). Type I collagen occupies about 90% of the organic parts of tissues, with the rest non-collagenous proteins (NCP), biopolymers, lipid, citrate, lactate, etc. NCPs include phosphophoryn, sialoprotein, glycoprotein, proteoglycan, osteopontin (OPN), osteocalcin, dentin matrix protein-1, osterix, and Cbfa1 (Runx2). These proteins are known to trigger the bone resorption and generation processes7-15.
Based on the potentials of osteoconduction, osteoinduction, and osteogenesis through growth factors in tooth and similar histogenesis between tooth and bone, a novel bone graft material can be developed utilizing the inorganic and organic components of an extracted tooth. Indeed, autogenous tooth bone graft material (AutoBT; Korea Tooth Bank Co., Seoul, Korea) has been developed from an extracted tooth. A non-restorable tooth or a third molar tooth is assigned to be extracted from the patient. With fabrication and demineralization process, AutoBT material is made from the extracted tooth. This AutoBT is grafted back to the same patient when guided bone regeneration is necessary in dental surgeries. Currently, AutoBT is widely used in clinics in Korea and Japan.
This review paper provides overviews of the chemical compositions of dentin due to its similarities to those of alveolar bone and previous studies on demineralized dentin matrix (DDM), an initial tooth-derived tissue engineering application. Finally, we summarized recent applications of tooth as bone grafting material.
II. Inorganic and Organic Components of Dentin
1. Hydroxyapatite, inorganic component
Dentin consists of 70% hydroxyapatite in its weight volume. Hydroxyapatite in dentin is structured with low-crystalline calcium phosphate16, making future bone remodeling possible. Bone tissues are also mainly composed of low-crystalline apatite. In contrast, hydroxyapatite in enamel is structured as high-crystalline calcium phosphate. High crystalline contents are not easily decomposed by osteoclasts, resulting in slow resorption and consequently poor osteoconductivity17.
2. Bone growth factors and type I collagen, organic component
Growth factors are signaling proteins that regulate cellular growth, proliferation, and differentiation18. Urist19 initially discovered BMPs and studied their roles in 1965. BMPs are known to exist in the bone matrix, osteosarcoma tissue, and dentin matrix, functioning to differentiate perivascular mesenchymal stem cells into cartilage and bone tissues20-23. Several studies have successfully isolated BMPs from dentin, enamel, and cementum of bovine, rats, guinea pigs, and rabbit teeth8,22-25. With extensive studies on BMPs, researchers have confirmed the osteoinductivity of BMPs extracted from animal teeth such as bovine, lapine, and murine teeth8-10,22,23,26-30.
Since only a limited amount of BMPs can be extracted from the teeth, however, the clinical utilization may be limited31-33. Therefore, various recombinant human BMPs (rhBMP) have been recently manufactured by gene recombination based on mammal cells or colon bacilli34-36.
Dentin and cementum contain various other growth factors besides BMPs such as insulin-like growth factor (IGF), platelet-derived growth factor (PDGF), fibroblast growth factor (FGF), and transforming growth factor (TGF)-β37,38. Finkelman et al.39 reported the extraction of TGF-β, IGF-I, IGF-II from human dentin but at lower levels compared to those from human bone.
About 90% of dentinal organic components are known to be type I collagens. These triple-helix structured collagens are the most abundant protein in vertebrates. Collagen-derived materials have demonstrated biocompatibility and interference in bone formation at the implanted sites40-42.
The rest of dentinal organic components are NCP. NCPs that contribute to mineralization are osteocalcin, osteonectin, phosphophoryn, dentin sialoprotein (DSP), dentin-specific extracellular matrix protein, etc. Phosphophoryn in particular, bound to type I collagen, contributes to the mineralization process; it is of the largest amounts among NCPs. Previous studies discovered through the immune-histochemical study that OPN and DSP manifested 6-8 weeks after grafting the tooth graft material on alveolar bone defects in Wistar rats43. OPN is known to trigger osteogenesis through the early differentiation of the osteoblasts but also leads to bone resorption by allowing adherence of osteoclasts to the bone surface. DSP has a significant role in dentin calcification12,44.
III. Backgrounds of Demineralized Dentin Matrix
1. Biocompatibility
Traditionally, roots were intentionally left for the prevention of alveolar bone resorption in removable prosthodontics or in cases of tooth extractions45,46. Intentional partial odontectomy has been safely practiced when roots of impacted third molar are situated close to the inferior alveolar nerve or ankylosed since only a crown portion is dissected, leaving the roots behind47. The root remnant of non-pathology involved tooth in alveolar bone does not induce any inflammatory response. Osteoclast cells appear in the pulp cavity, with the pulp replaced by bone, followed by root resorption. After all, the remaining roots completely fuse with the surrounding alveolar bone. Based on these clinical reports, alveolar bone and teeth can be inferred to have high level of affinity to each other48-50.
Homogenous demineralized dentin matrix (HDDM) is as an effective biocompatible bone graft material as autogenous demineralized dentin matrix (ADDM) since it induces heterotopic bone formation with no host immune rejection51,52. The demineralization process of HDDM does not denature osteopromotive properties. HDDM is a reservoir of biochemical factors that induce cellular proliferation as well as cell differentiation and chemotaxis53,54. In the histomorphometric analysis of HDDM in vitro, HDDM resorbs itself during the bone remodeling process53. Gomes et al.54 further evaluated the bone repair process after implantation of HDDM slices in surgical defects created in the parietal bones of rabbits with alloxan-induced diabetes. They reported that HDDM was biocompatible, stimulating bone tissue formation. In this study, HDDM is well accepted by the host and is totally incorporated into newly formed bone tissue.
2. Osteoinduction and release of bone morphogenic protein
Highly soluble, BMPs do not exert osteoinductive effects when used alone. Scaffolds are used to force BMPs to stay at the implant site55-57. Scaffold functions as carrier. An ideal scaffold should control-release growth factors or cells and can prevent degradation and inactivation18. Different materials are used for different purposes. Collagen and TCP are clinically used most widely58. For the delivery of BMPs and growth factors, collagen, calcium phosphates, and polyesters such as polycaprolactone have been used59-61.
DDM was introduced as an alternative material for scaffold in releasing BMPs62-64. Ike and Urist62 suggested that root dentin prepared from extracted teeth could be recycled for use as carrier of rhBMP-2. Although the quantity of endogenous BMP in dysfunctional teeth is very small or nil, active new bone formation was observed by many scientists when DDM was used as carrier62,64. According to the biochemical and histomorphometric analyses of bone and cartilage induced by human DDM and BMP-2, researchers concluded that human DDM of vital teeth origin induced bone and cartilage, and that BMP-2 strongly accelerated bone formation in the DDM carrier system65.
3. Demineralization
The demineralization process is required for freeing the various growth factors and proteins, since the release of the growth factors is sometimes blocked by the presence of hydroxyapatite crystals. Many authors observed that heterotrophic bone was induced when DDM was grafted in the lapine, porcine, and murine muscle tissues. As such, decalcification of dentin is believed to induce the release of BMP, thereby leading to osteoinduction52,66-70. Researchers use various decalcification methods. Decalcified dentin and bone using 0.6N HCl lead to the inducement of connective tissue cells and formation of endochondral bone in muscle and in skin connective tissues19,66,71-75. Ike and Urist62 partially demineralized the roots of the teeth using 0.6N HCL for 24 hours, and then cut them in 0.5 g blocks to produce partially demineralized matrix (PDM). PDM was then washed in cold water and lyophilized. An alternative approach was employed by Inoue et al.67; they grafted the demineralized dentin tissues using 0.6N HCL (pH1) and 3M (9N) in the rectal abdominis muscles of Wistar rats. Inoue et al.67 reported favorable chondrogenesis and osteogenesis, with the HCL-demineralized dentin showing relatively superior results. Different approaches in acid treatment protocols were used. DDM was treated using 2% HNO3. Several animal studies showed favorable results, with observed new bone formation68,76.
Some studies showed contrary results. According to Ike and Urist62, when human partially demineralized dentin granules were grafted in the intramuscular pockets, osteoinduction was not observed. Based on the quantitative analysis of proliferation and differentiation of the MG-63 cell, however, cellular adhesion and proliferation activity of the MG-63 cell on partially demineralized dentin matrix were noted77. With differently employed methods, one may conjecture that the osteoinductive properties of dentin may depend on different acid treatment protocols.
IV. Human Tooth as Graft Material
Bone substitutes have been actively used in clinics to reconstruct bony defects. There are four categories of bone graft materials: autograft, allograft, alloplast, and xenograft. With four types of graft materials available, the use of these materials depends on clinical applications, volume of deficiency, and evidence-based studies52,78,79. Above all, autografts are known to be the gold standard due to its osteoinductivity, osteoconductivity, and osteogenicity. Still, autogenous bone grafts harvested from extra-oral sites have some limitations, such as high morbidity, potential resorption, and high costs78,80. With advancements in tissue engineering, researchers have extensively studied compensating the drawbacks of autografts. Thus, many researchers paid attention to human tooth as one of the intraoral donor sites due to its chemical similarities to bone.
1. Autogenous demineralized dentin matrix
Extensive studies in vitro have been conducted on ADDM with its biocompatibility, osteoinductivity, and osteo conductivity81-84. In animal studies, ADDM induced bone formation according to the histology analysis81-83. For instance, Gomes et al.54 performed a histological evaluation of the osteoinductive property of ADDM on calvarial bone defects in rabbit. According to the study, ADDM was verified to have chemotactic properties for osteoprogenitor cells and osteoblasts, promoting the acceleration of bone repair process at the bony defect. Slices of ADDM induced direct bone formation, and they were incorporated by the newly formed bone tissue and remodeled82.
The mechanisms involved in the osteogenesis of ADDM include endochondral and intramembranous bone formation52,85-87. Likewise, the osteogenesis of ADDM is influenced by the size and form of graft materials87. The ideal sizes of graft material granules are different from author to author, ranging from 75 µm to 500 µm73,88,89. Some authors reduced the inter-particulate distances by adding β-TCP due to difficulties in homogenizing the sizes40. Since ADDM contains native growth factors supporting mesenchymal cell attachment and further absorbs several proteins derived from body fluid, however, some authors state that homogenizing the ADDM granule size is not critical65,90.
The clinical effectiveness of ADDM was tested in pocket preservation. Wistar rat's incisors were frozen soon after extraction, and then milled with hydroxypropyl cellulose added. Consequently, early healing and bone formation in the extraction socket were observed when grafted with milled tooth. This study used the extracted tooth as a whole without decalcification, including both enamel and dental pulp. Therefore, the results indicate that osteoinductive healing may come from growth factors in dentin or dental pulp91. Another study was conducted on the human third molar socket wherein the greater homogeneity of bone radiopacity with enhanced healing process was observed53,81,84. Periods of radiographic observation focusing on the changes in radiopacity and in the peripheral boundary between graft material and bone and clinical observations confirmed that the graft was biocompatible and clinically easy to use92. Another application of ADDM is on implant dentistry. In fact, ADDMs have been actively tested in implant osseointegration and bone remodeling capacity; thus enhancing implant primary stability86.
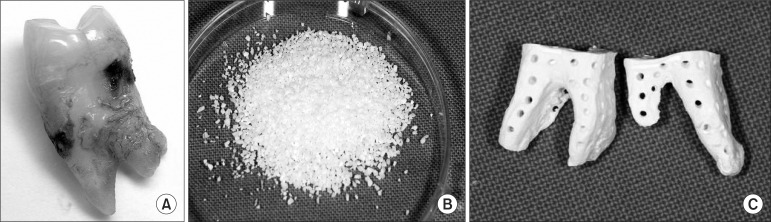
Based on decades of research and scientific facts on tooth, Jeong et al.80 and Kim et al.93 suggested that AutoBT is an excellent alternative to autogenous bone graft. After all, AutoBT was developed and has been in clinical use since 2008 in Korea. With the patient's consent, the extracted teeth are sent to Korea Tooth Bank in 75% ethyl alcohol storage container.(Fig. 1. A) After dissection of the anatomical crown, sample root portions are ground into powder form, with each particle measuring 400-800 µm in diameter.(Fig. 1) The remaining soft tissues and contaminants of the particulate AutoBT are removed with distilled water. Once subjected to dehydration, defatting, lyophilization, and ethylene oxide sterilization processes, AutoBT is packed. A block form of AutoBT is fabricated in the same manner as particulate bone graft excluding the grinding steps.(Fig. 1. C)
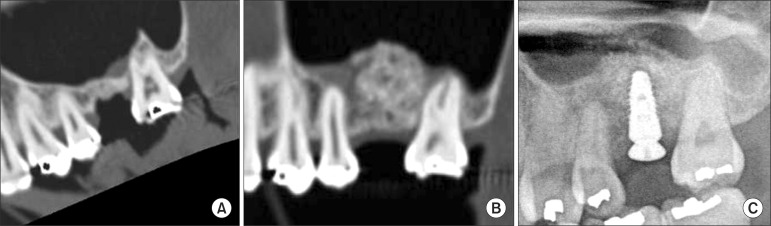
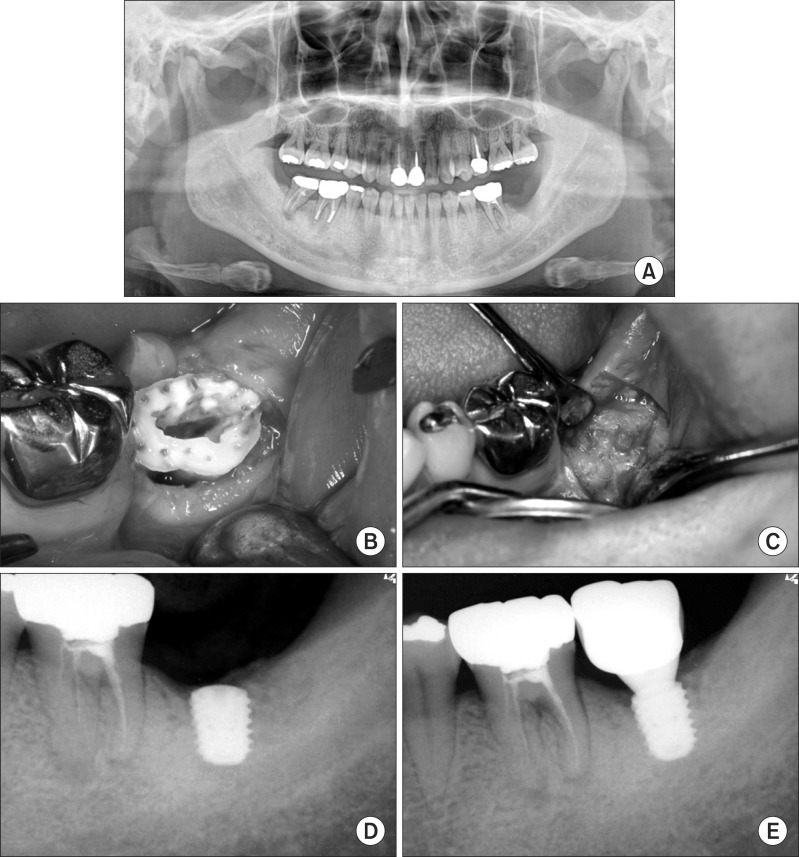
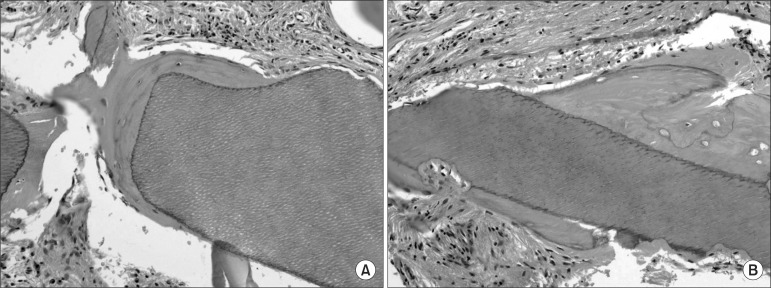
The basic components and surface structure of AutoBT have been analyzed using X-ray diffraction analyzer, scanning electron microcopy, and histomorphometric evaluation16,78. AutoBT consists of low-crystalline hydroxya-patite and other calcium phosphate minerals such as TCP, ACP, and OCP, which are components similar to those of human bone16. With the analysis of AutoBT's basic components, diverse clinical applications of using AutoBT have been identified, supporting the osteoinductive and osteoconductive capabilities of AutoBT with favorable clinical results79,94-103. In clinical studies, AutoBT has been grafted in sinus bone graft (Fig. 2. A-2. C), guided bone regeneration, ridge augmentation, ridge splitting, and socket preservation94-103.(Fig. 3. A-3. E) Later, researchers histologically noticed that AutoBT underwent gradual resorption, and that it was replaced by new bone16,78.(Fig. 4. A-4. B) AutoBT can also be mixed with other types of bone graft materials when repairing large defects104. Furthermore, the block form of AutoBT is an excellent choice as material when reconstructing large bony defects with or without the combination of AutoBT powder types102. The block form of AutoBT is fabricated with the same procedures as the powder type except crushing the teeth. Thus, the AutoBT block form still includes the remaining root structure of the extracted tooth.
With support from the previous studies on AutoBT, it was confirmed that AutoBT is a safe and effective bone graft material. AutoBT was further suggested to have potential to be developed into allogenic and xenogenic tooth bone graft materials, ideal scaffold for stem cells and bone growth factors, and endodontic and tooth restorative material.
V. Conclusion
Indeed, DDM has shown potential applications in bone substitute and scaffold. As discussed in this review, ADDM, with absence of antigenicity, enhances bone-remodeling capabilities. Among a variety of available bone graft materials, choosing the appropriate one is challenging. While choosing the graft material should be dictated by the extent of defects and the procedural purposes, tooth-derived bone graft may be considered as an option given its autogenous origin and favorable clinical and histological outcomes when teeth extraction is necessary. Further studies are needed in evaluating clinical efficacies and comparing other commercially available bone graft materials.
 XML Download
XML Download