

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
YKL-40, also referred to as cartilage glycoprotein-39 or chitinase-3-like-1 (CHI3L1), is a member of the mammalian chitinase-like protein family; its abbreviation is derived from the one-letter code for the first three N-terminal amino acids, tyrosine (Y), lysine (K), and leucine (L), and its molecular weight (40 kDa) [123]. YKL-40 is expressed in a variety of cells, including some primary immune cells such as macrophages and neutrophils, chondrocytes, fibroblasts, and some cancer cells [3]. Although the exact roles of YKL-40 remain unclear, it has been implicated in diverse biological processes such as extracellular matrix remodeling, fibrosis, angiogenesis, and inflammation [4]. Elevated levels of YKL-40 have been observed in patients with acute or chronic inflammatory diseases such as cancers, and in those with cardiovascular, infectious, and autoimmune diseases [5]. In particular, a few previous studies have suggested that YKL-40 might be a site-specific inflammatory marker given that it is locally produced at the sites of inflammation [6789].
Urinary tract infection (UTI) is one of the most common bacterial infections in children. Notably, febrile UTI may cause pyelonephritis and subsequent renal scarring [10]. Therefore, it is important to diagnose and treat febrile UTI promptly. However, in some cases, the diagnosis of febrile UTI in young children is difficult because of the lack of specific symptoms in a considerable proportion of young children. Moreover, several practical problems such as collecting appropriate urine samples and discriminating between insignificant pyuria or bacteriuria from a true UTI can hinder making an accurate diagnosis of UTI in infants [11]. As a result, clinicians may be confused as to whether patients should be treated with antibiotics or if imaging methods are necessary for evaluating UTI-associated urological anomalies, especially before obtaining the results of urine culture to confirm an infection. Therefore, more specific markers of UTI besides abnormal urinalysis results are needed. Previous studies have suggested several potential biomarkers for this purpose, including procalcitonin, interleukin (IL)-8, IL-6, neutrophil gelatinase associated lipocalin, and kidney injury molecule-1 for detecting UTI, vesicoureteral reflux (VUR), or renal scarring [121314]. However, little information has been obtained regarding the association between YKL-40 and UTI. Here, we examined the association between urinary YKL-40 levels and UTI in febrile young children.
METHODS
1. Patients
In total, 79 children (age range, 2–24 months; 47 male and 32 female infants) who had a fever higher than 38℃ were admitted to the Department of Pediatrics at the Catholic University of Korea, Bucheon St. Mary's Hospital, between March 2013 and January 2015. These patients were divided into two groups according to their urine culture results: a UTI group (n=44) and a control group (n=35). Febrile children with positive urine culture results showing pure growth of 105 colony-forming units/mL on a catheterized specimen were included in the UTI group. Patients using antibiotics before visiting the hospital were excluded. Febrile children with a negative urine culture were included in the control group. The causes of fever in the control group were as follows: influenza viral infection (n=7), respiratory syncytial virus infection (n=6), adenovirus infection (n=3), bocavirus infection (n=2), rhinovirus infection (n=1), coronavirus infection (n=1), parainfluenza viral infection (n=1), and other viral infections such as exanthem subitum and herpangina (n=14).
2. Laboratory and radiological evaluation
Laboratory examinations, including white blood cell (WBC) counts, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), routine biochemical analysis, urinalysis with microscopy, and urine culture were obtained before initiating antibiotic therapy. Pyuria was defined when ≥5 WBCs were detected, and hematuria was defined when ≥5 red blood cells were detected in a high-power field based on microscopic urinalysis. Proteinuria was defined when a protein score ≥+1 (+1 to +4) was obtained in urinalysis. The estimated glomerular filtration rate (eGFR) was calculated using a revision of the Schwartz equation: 0.413× height (cm)/serum creatinine (Cr) (mg/dL). All febrile patients with UTI underwent renal sonography and technetium 99m-labeled dimercaptosuccinic acid (DMSA) imaging at the time of diagnosis. Voiding cystourethrography (VCUG) was indicated, if the ultrasonography or DMSA imaging (or both) result was abnormal; for example, if hydronephrosis or ureteral dilatation was found on ultrasonography or a photon defect was detected in DMSA imaging. Hydronephrosis was defined according to the Society for Fetal Urology classification [15]. In total, 24 patients with UTIs (54.5%) underwent VCUG after their fever subsided and urine culture produced negative results.
3. Urinary YKL-40 measurements
Samples for measuring urinary YKL-40 levels were obtained from the children upon routine urine collection for culture. Samples were centrifuged at 4℃ for 15 minutes at 3,000×g within 30 minutes of collection and stored at -80℃ until final analyses were conducted. Urinary levels of YKL-40 were measured using ELISA kits for human CHI3L1 (R&D Systems, Minneapolis, MN, USA), according to the manufacturer's instructions. All samples were run in duplicate, and mean values were presented. The respective inter- and intra-assay precision values were 4.3–4.7% and 5.3–6.9%, respectively. The standard curve range for the assay was 62.5–4,000 pg/mL, and the detection limit for YKL-40 was 3.55 pg/mL. While the majority of samples were within the range of the standard curve, urinary YKL-40 levels for some control subjects were below the detectable range, which is consistent with a previous report [16]. Accordingly, YKL-40 values below the detection limit were approximated to 1.775 pg/mL (the mean value between 0 and the lower limit of detection), and urinary levels of YKL-40 were normalized to the urinary Cr level. The urinary concentrations of biomarkers, including urinary YKL-40, is inversely proportional to the urinary flow rate for a given amount of a total excreted biomarker. Because urinary Cr excretion is relatively constant in the case of normal renal function, the urinary Cr level reflects the urinary flow rate. Therefore, we expressed the concentration of urinary YKL-40 as the urinary YKL-40-to-Cr ratio (urinary YKL-40/Cr) [1718]. The study was approved by the institutional review board at Bucheon St. Mary's Hospital, the Catholic University of Korea, and written informed consent was obtained from the parents of all participating children.
4. Statistical analysis
Data are presented as the mean±SD for normally distributed values and as the median and interquartile range for non-parametric values. Differences between the two groups were analyzed by unpaired Student's t-tests (parametric distributions) or Mann–Whitney U test (non-parametric distributions). To assess the diagnostic value of urinary YKL-40 for detecting UTI, we conducted an ROC curve analysis and calculated the areas under the ROC curves (AUCs) with 95% confidence intervals. The associations between urinary YKL-40 levels and the clinical parameters were analyzed using Spearman's correlation coefficient r. Statistical analyses were performed using SPSS Statistics for Windows (version 20.0; IBM Corp., Armonk, NY, USA) and MedCalc for windows, version 15.4 (MedCalc Software, Ostend, Belgium). Values of P<0.05 were considered to indicate statistical significance.
RESULTS
1. Baseline characteristics, and laboratory and radiological data of subjects
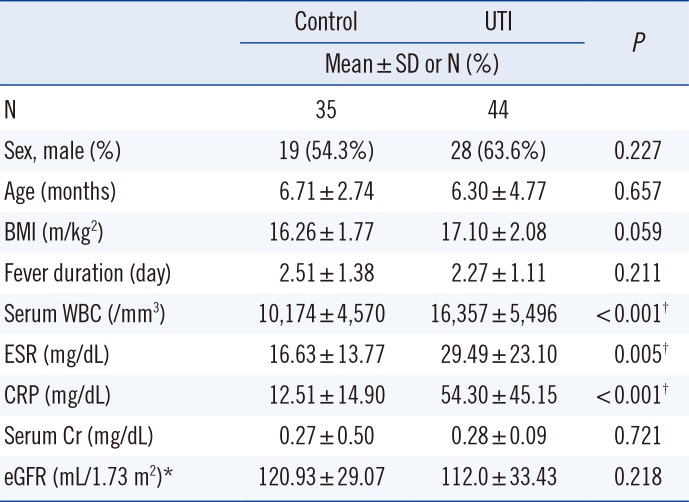
As shown in Table 1, the sex distribution, age, fever duration, body mass index (BMI), and eGFR did not differ between the control and UTI groups. However, WBC counts, ESR, and CRP levels of children in the UTI group were significantly higher than those in the control group. Remarkable counts of Escherichia coli and Klebsiella pneumoniae (>105 colony-forming units/mL) were noted in the urine culture of 42 (95%) and two (5%) of the children in the UTI group, respectively. Among the children with UTI, 18 (40.9%) showed positive nitrite and 15 (34.1%) showed proteinuria in the initial urinalysis, and 43 (97%) showed pyuria and 12 (27.3%) showed hematuria by microscopy. Among the children in the control group, nine (25%) had pyuria. In the UTI group, 35 children (80%) showed a photon defect in DMSA imaging and eight (18%) showed hydronephrosis in renal sonography. Eight children (18% of UTI group and 33% of children undergoing VCUG) showed VUR (Table 2).
2. Urinary YKL-40/Cr values of subjects
The urinary YKL-40/Cr values were significantly higher in the UTI group than in the control group. The median (interquartile range) values of urinary YKL-40/Cr in the UTI and control groups were 783.83 pg/mg (132.62–18,015.0 pg/mg) and 15.30 pg/mg (7.01–25.28 pg/mg), respectively (P<0.001).
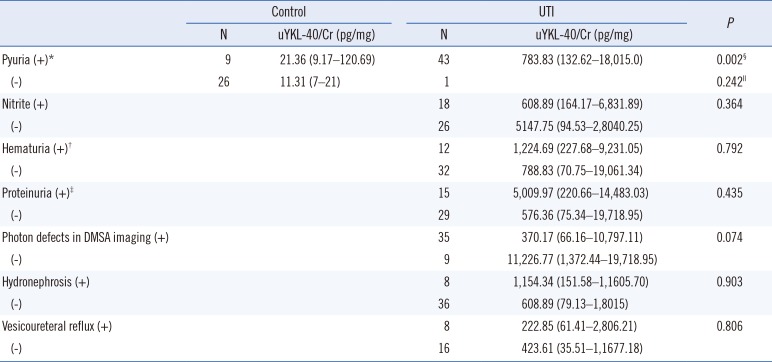
Table 2 shows the urinary YKL-40/Cr levels according to the findings of urinalysis and imaging studies of the children. Based on the presence or absence of pyuria, the levels of urinary YKL-40/Cr were significantly higher in children in the UTI group than in those in the control group who had pyuria; however, there was no difference according to the presence or absence of pyuria in the control group. The urinary YKL-40/Cr levels among children with UTI did not differ according to other urinary abnormalities; that is, the presence of hematuria, proteinuria, or positive nitrite. In addition, the levels did not differ according to the results of imaging studies; that is, regardless of whether or not photon defects were found in DMSA imaging, hydronephrosis, or VUR.
3. Diagnostic value of urinary YKL-40/Cr for the detection of UTI
ROC curves were analyzed to compare the diagnostic value of urinary YKL-40/Cr with abnormal urinalysis findings (pyuria and positive nitrite) for detecting UTI (Table 3). The AUC for urinary YKL-40/Cr was 0.881. The best cut-off value of 125.23 pg/mg for urinary YKL-40/Cr had a sensitivity of 75% and a specificity of 91.43%. The AUCs for positive pyuria and positive nitrite for detecting UTI were 0.860 and 0.705, respectively. The AUC for both positive pyuria and positive nitrite was 0.693.
4. Correlations between urinary YKL-40/Cr and other clinical variables
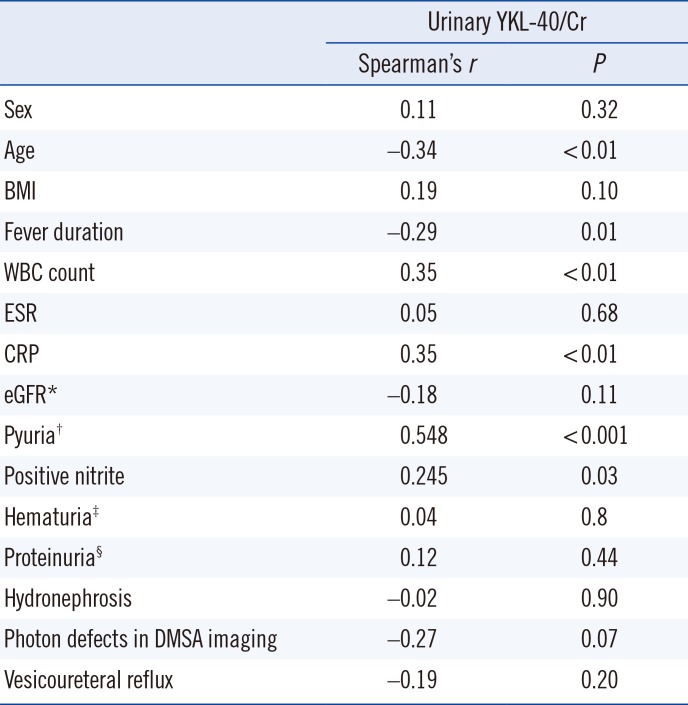
As summarized in Table 4, the levels of urinary YKL-40/Cr were positively associated with WBC count, CRP levels, pyuria, and positive nitrite, and negatively associated with fever duration, and age. No association was found with any other clinical parameters, including sex, BMI, eGFR, hematuria, proteinuria, or abnormalities detected on imaging.
DISCUSSION
The present study showed that the levels of urinary YKL-40/Cr were elevated in febrile young children with UTI compared with sex- and age-matched children with fever without UTI. According to the ROC curve analysis, the diagnostic value of urinary YKL-40/Cr for detecting UTI appears to be higher than that of pyuria or nitrite.
Urine culture is the standard test for detecting UTI [19]. However, it takes several days to obtain the results of urine culture for confirming an infection. In the case of febrile UTI, treatment delayed by more than 48 hr may cause deleterious effects such as renal scarring [20]. Therefore, clinicians may often make decisions to prescribe antibiotics or perform renal sonography based on the findings of initial urinalysis. However, previous studies have shown that positive urinalysis findings and/or positive urine culture may not reflect a true case of UTI. A considerable portion of patients with UTIs determined by positive urine culture may have negative urinalysis findings; alternatively, some patients without UTIs but with viral infections may have abnormal urinalysis findings such as pyuria, asymptomatic bacteriuria, or both [1121]. Therefore, patients with false-positive findings run the risk of receiving unnecessary antibiotic treatments and undergoing imaging. By contrast, patients with false-negative findings run the risk of delayed treatment.
In the present study, nine children in the control group had pyuria. When applying a cut-off value of 125.23 pg/mg to the urinary YKL-40/Cr level for indicating UTI in these patients, eight of the nine subjects in the control group with pyuria showed urinary YKL-40/Cr levels<125.23 pg/mg. Furthermore, the levels of urinary YKL-40/Cr of the children with pyuria in the control group were significantly lower than those in the UTI group, although the levels were not different from those without pyuria in the control group (Table 2). Based on these results, we suggest that the level of urinary YKL-40/Cr may help distinguish UTI from viral infections, when pyuria is detected without a positive nitrite result. This assessment can help avoid unnecessary antibiotic treatments and imaging for patients with false-positive findings. However, the one patient in the UTI group who showed no pyuria or positive nitrite had a urinary YKL-40/Cr level>125.23 pg/mg, and photon defects were detected in the DMSA scan. Recently, Kim et al [22] also showed that 50% of febrile infants who had a significant culture of uropathogens but did not have pyuria or nitrite detected in urinalysis showed photon defects on the DMSA scan, and 33.3% of the patients had underlying urological abnormalities such as vesicoureteral reflux and obstructive uropathy. In these clinical scenarios, the measurement of urinary YKL-40/Cr levels may help detect UTI in patients with false-negative findings.
YKL-40 is involved in local inflammation by being produced and activated in the injured tissue. Tran et al [8] showed that YKL-40 plays a role in promoting the onset of bacterial infectious colitis in a murine model of intestinal infection. Specifically, they showed that YKL-40 helps the bacteria to adhere to intestinal epithelial cells and to invade the lamina propria, where it synergistically cooperates with IL-6 to activate the STAT3 signaling pathway in a nuclear factor-kappa B (NF-κB)- and mitogen-activated protein kinase (MAPK)-dependent manner. Tang et al [7] further suggested an association between YKL-40 and the inflammation of asthma by showing that YKL-40 induced IL-8 expression from the bronchial epithelium via MAPK- and NF-κB-dependent-pathways, subsequently stimulating the proliferation and migration of bronchial smooth muscle cells. Moreover, elevated tissue levels of YKL-40 have been observed in patients with osteoarthritis and with central nervous system and pulmonary infections, and these levels correlated with disease severity [6923]. Recently, urinary YKL-40 has been suggested as a marker for reflecting renal injury. Shmidt et al [24] showed that CHI3L1 mRNA expression was upregulated in kidney macrophages in a murine model of renal ischemia/reperfusion injury, with increased levels of Brp-39, the mouse ortholog of human YKL-40, in the urine. They also showed that Brp-39 stimulated intracellular activation of the PI3K/Akt pathway in renal tubular cells, resulting in decreased apoptosis. In addition, urinary YKL-40 levels tend to be increased in patients with diabetic nephropathy and acute kidney injury, and in kidney transplant recipients with delayed graft function [242526]. This evidence suggests that YKL-40 may be locally produced in injured tissues and may modulate inflammatory processes and limit tissue degradation [82324]. However, to our knowledge, the association between YKL-40 and UTI has not yet been evaluated. In the present study, the levels of urinary YKL-40/Cr were higher in febrile young children with UTI than in age-matched children with fever from other causes. The level of YKL-40 was positively associated with other inflammatory markers, such as the WBC count and CRP level, but not with imaging abnormalities reflecting renal injury. We suggest that urinary YKL-40 may be a marker of local inflammation in febrile children with UTI. However, we cannot exclude the possibility that the increased levels of urinary YKL-40 may also reflect the systemic inflammation in UTI patients, because we did not examine the levels of serum YKL-40. In addition, the present study included only a relatively small number of subjects. The study was also limited by its cross-sectional design. Therefore, to confirm the role of urinary YKL-40 as a marker for local inflammation in febrile children with UTI, further studies including longitudinal observations in a larger population, and investigations of other urinary inflammatory markers such as IL-6 or IL-8 as well as serum YKL-40 are needed.
In conclusion, to our knowledge, this is the first report demonstrating an association between urinary YKL-40 and UTI in febrile young children. There is a continuing need for identifying more specific markers of UTI besides relying on abnormal uri-nalysis results. Toward this goal, the present results suggest that the urinary YKL-40 level may help identify a true case of UTI as an adjuvant method to standard urinalysis, especially for febrile infants who have false-positive or -negative findings. In addition, as a urinary biomarker, YKL-40 has a particular advantage for young children, because urine can be collected in a non-invasive manner. Further studies are warranted to investigate the pathophysiological role of urinary YKL-40 in the development of UTI in order to elucidate its value as a diagnostic and therapeutic target for infants with febrile UTI.

 XML Download
XML Download