

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Mucormycosis (previously described as zygomycosis) is an emerging opportunistic infection caused by fungi belonging to the order Mucorales [1]. Mucormycosis, which was once considered a rare disease, is now one of the most common invasive mold infections in patients with hematologic malignancies, second only to aspergillosis [2], and in immunocompetent hosts [3]. Mucorales fungi can be easily differentiated from Aspergillus fungi on culture. However, sometimes it is difficult to differentiate them on the basis of the results of imaging studies and histopathological analysis. Accurate identification is critical for treatment because these fungi cause two different infections. Amphotericin B (AMB) and azole are the best drugs for treating mucormycosis and aspergillosis, respectively. Overall mortality rate associated with mucormycosis is >47% [34]. Therefore, rapid and accurate diagnosis and treatment of mucormycosis are essential for positive prognosis [5]. Unfortunately, identification of Mucorales fungi by conventional methods is demanding. In this study, we comparatively identified Mucorales fungi by using phenotypic and molecular identification methods.
We analyzed 12 Mucorales isolates that were collected from Samsung Medical Center, Seoul, Korea, during 2010-2014. Fungal isolates that were repeatedly isolated from a single patient or from patients with suspected invasive fungal infections and that were morphologically identified as Mucorales were also included in the study. Contaminants growing on the edge of culture plates away from inoculation sites were excluded. Clinical specimens were inoculated on Sabouraud dextrose agar and were cultured at 30℃ for initial three days and at room temperature (23-26℃) thereafter. Isolates were identified by using phenotypic characteristics such as growth rate, colony morphology, and reproductive structures [6]. Scotch tape method and lactophenol cotton blue stain were used for slide preparation. DNA was extracted by using MagNa Pure LC DNA Isolation Kit (Roche Diagnostics, Mannheim, Germany) or I-genomic BYF DNA Extraction Mini Kit for fungi (iNtRON Inc., Seongnam, Korea), according to the manufacturer's recommendations. Briefly, 5-10 mg of mycelium was mixed with phosphate-buffered saline and vortexed. The sample was mixed with proteinase K, incubated at 95℃ for 10 min, and cooled. DNA was isolated by using magnetic bead technology according to the manufacturer's instructions. The isolated DNA was amplified in a thermal cycler (Model 9700; Applied Biosystems, Foster City, CA, USA), and amplified products were sequenced by using BigDye Terminator Cycle Sequencing Ready Reaction Kit (Applied Biosystems) and ABI Prism 3100 Genetic Analyzer (Applied Biosystems). Internal transcribed spacer (ITS) was amplified by using primer sets ITS-1/ITS-4 and ITS-5/ITS-4, and D1/D2 region of the 28S subunit of ribosomal DNA was amplified by using primer set NL-1/NL-4, as proposed in CLSI guidelines [7]. Sequences obtained were used to perform BLAST search in the GenBank database available at the NCBI website (http://www.ncbi.nlm.nih.gov). Outputs were sorted on the basis of percentage identity and were considered significant at ≥98% identity and ≥90% query coverage. Isolate were considered as misidentified if their phenotypic identification was different from their molecular identification at the genus level.
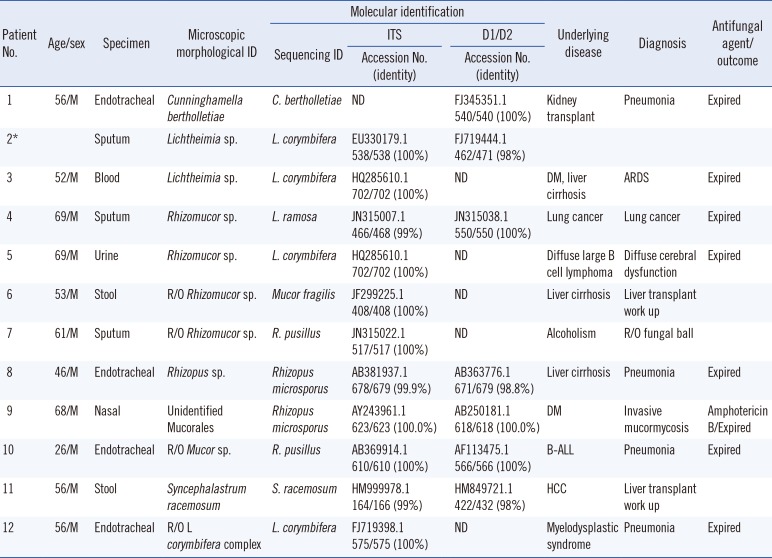
Five isolates were identified as Lichtheimia spp., (formerly Absidia spp.; four Lichtheimia corymbifera isolates and one Lichtheimia ramosa isolate) on the basis of DNA sequencing analysis. Further, two Rhizopus microsporus isolates, two Rhizomucor pusillus isolates, one Cunninghamella bertholletiae isolate, one Mucor fragilis isolate, and one Syncephalastrum racemosum isolate were identified. Results of phenotypic and molecular identification are listed in Table 1. Discrepancy between phenotypic and molecular identification at the genus level was observed for four isolates. Of these, three isolates initially identified as Rhizomucor on the basis of phenotypic identification were re-classified as Lichtheimia (L. ramosa and L. corymbifera) and Mucor (M. fragilis) on the basis of molecular identification. One isolate initially identified as Mucor was re-classified as Rhizomucor (R. pusillus) on the basis of molecular identification. One unidentified Mucorales isolate was classified as Rhizopus microspores on the basis of molecular identification. One patient (no. 9) was diagnosed as having invasive fungal infection on the basis of histopathological analysis. Concordance rate between phenotypic and molecular identification was 58.3% (7/12). Further, ITS and D1/D2 analyses provided more effective results.
Kontoyiannis et al. [8] identified 20 Mucorales isolates, with 20% error rate for phenotypic identification compared with molecular identification. In contrast, Alvarez et al. [9] reported 100% concordance rate between phenotypic and molecular identification at the genus level. A study by Jang et al. [10] in Korea compared phenotypic and molecular methods for identifying mold; however, only 9% of all isolates tested were Mucorales (four isolates). Some species such as Cunninghamella and Syncephalastrum can be identified easily on the basis of their morphology. Rhizopus spp. can be easily identified on the basis of the presence of rhizoids and striated or grooved sporangiospores. However, identification of Rhizomucor, Lichtheimia, or Mucor spp. based on their morphological characteristics is difficult. In the present study, isolates 4, 5, and 6 were morphologically identified as Rhizomucor because they had round sporangia compared with pear-shaped sporangia of Lichtheimia. Isolate 9 could not be classified as Mucorales because its rhizoids and sporangia were not observed. Because no rhizoids were observed in isolate 10, it was classified as Mucor. Absence of rhizoids is the key to differentiate Mucor spp. from other Mucorales fungi. However, this is not always applicable because of some exceptions such as that observed above. This explains the low concordance rate between phenotypic and molecular identification. Therefore, molecular identification of Mucorales fungi is more reliable than phenotypic identification [111213]. ITS and D1/D2 analyses performed in this study provided comparable performances. However, as DNA targets, ITS and D1/D2 regions were not superior to each other. Because ITS shows increased level of demarcation in some species while D1/D2 region shows increased level of demarcation in other species, they are considered complementary.
Mucorales fungi show variable susceptibility to antifungal drugs. Rhizopus spp. are less susceptible to itraconazole, posaconazole, and AMB than Lichtheimia spp. and less susceptible to AMB than Mucor spp. [1]. Of 4,011 fungal isolates collected in this institute during the study period, 23.5% belonged to Aspergillus spp. and 0.7% belonged to Mucorales. Mucorales fungi cause a small portion of fungal infections. However, antifungal susceptibility testing of Mucorales fungi has provided limited data. Prompt treatment of mucormycosis is important because it is associated with high mortality rate, as evidenced by Chamilos et al. [5] who showed that delaying AMB-based treatment for >6 days after the onset of mucormycosis symptoms increased mortality rate by two fold (compared with previous treatments) and decreased survival rate to <20% at 12 weeks after diagnosis. Although the isolates identified in this study were repeatedly recovered from immunocompromised patients, these patients did not have systemic mucormycosis. Therefore, the possibility of contamination cannot be excluded, especially for urine or stool specimens.
In conclusion, phenotypic differentiation and identification of Mucorales are difficult because different Mucorales share similar morphology. Molecular identification methods were effective for identifying Mucorales fungi. In addition, this study is noteworthy because it identified all medically important Mucorales fungi reported in Korea by using phenotypic and molecular identification methods.
 XML Download
XML Download