

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Stickler syndrome is a hereditary connective tissue disorder of collagen associated with ocular, orofacial, auditory, and musculoskeletal manifestations [1]. Patients with Stickler syndrome have a high risk (50-70%) of developing rhegmatogenous retinal detachment (RRD) because of retinal breaks [23]. Therefore, early diagnosis is important to prevent visual loss from RRD.
Stickler syndrome type 1 (STL1; MIM 108300) is caused by mutations in COL2A1, which is located on 12q13.11 and encodes type II collagen found in cartilaginous tissue and vitreous humor [1]. STL1 has characteristic membranous vitreous anomaly and presents with multi-system abnormalities [4]. Recently, the ocular-only variant of STL1 (OSTL1; MIM 609508) has been reported to have a high risk of RRD, but with minimal or absence of systemic involvement [15]. Mutations involving exon 2 of COL2A1 are characteristic of OSTL1 [256]. We report the first genetically confirmed cases of OSTL1 in Korea with two novel mutations in COL2A1.
CASE REPORT
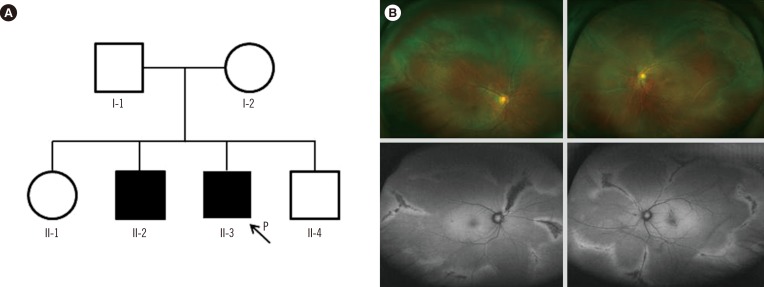
In family A, the proband (II-3, Fig. 1A) was a 39-yr-old man who visited the retina clinic for a regular check-up. His uncorrected visual acuity was 20/20 (right) and 20/25 (left). The fundus displayed radial perivascular atrophy, peripheral vitreous condensation, and a vitreous membrane (Fig. 1B). His older brother (II-2) had a history of retinal surgeries due to RRD in both eyes. His parents could not be examined but had no history of ocular disease, including retinal detachment, and there were no remarkable findings in other systems. The proband received prophylactic cryotherapy in both eyes to prevent RRD.
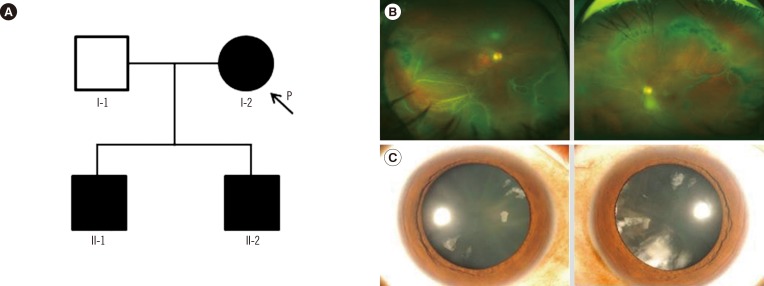
In family B, the proband (I-2, Fig. 2A) was a 57-yr-old woman who presented with sudden visual loss in the right eye. Her best-corrected visual acuity was finger counting in the right eye, and 20/20 in the left eye. Fundus examination revealed RRD with multiple retinal tears in the right eye (Fig. 2B). Vitreous membrane and radial perivascular atrophy were observed in both eyes. No systemic abnormalities were seen. Her first son (II-1; 35-yr) was myopic and had quadrantic lamellar cortical opacity (Fig. 2C). Radial perivascular atrophy was also seen; however, there were no retinal breaks. The second son (II-2) had history of retinal surgeries due to bilateral RRD. Prophylactic cryotherapy was performed in the non-detached eyes of the proband (I-2) and her first son (II-1).
After obtaining informed consent, genomic DNA was extracted from peripheral blood leukocytes of probands and their available family members. PCR and sequencing were performed by amplifying all coding exons of COL2A1 on the ABI 3730xl analyzer (Applied Biosystems, Foster City, CA, USA) using BigDye Terminator v3.1 Cycle sequencing kit (Applied Biosystems). Sequences were analyzed by comparison with the reference sequence of COL2A1, NM_001844.4. In family B, the second son (II-2) of the proband refused the genetic test.
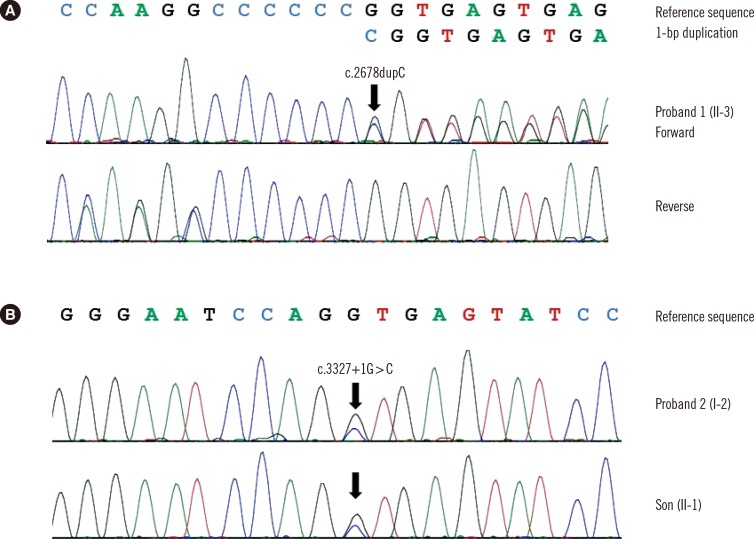
The proband of family A (II-3) was found to be heterozygous for a frameshift variant of COL2A1 (c.2678dupC; p.Ala895Serfs*49) with mutation in exon 40 (Fig. 3A). The other affected individual (II-2) refused the genetic test. In family B, the proband (I-2) was heterozygous for a novel variant (c.3327+ 1G>C) with mutation in intron 47 (Fig. 3B). The family study revealed that her first son (II-1) was heterozygous for the variant. Identified variants, c.2678dupC and c.3327+1G>C, were predicted to be truncating variants. These variants were absent from the Single Nucleotide Polymorphism Database (dbSNP), Exome Sequencing Project database, and in-house collection of 150 control exomes of Korean descent. We regarded them as likely pathogenic variants that may cause OSTL1 according to the standards and guidelines of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology [7].
DISCUSSION
Here we present two cases of OSTL1 carrying two likely pathogenic variants of COL2A1. Although several Korean STL1 cases with COL2A1 mutations have been reported [8910], these are all typical STL1 with musculoskeletal anomalies. In this study, all patients had ocular characteristics consistent with STL1, but systemic features were absent. This is the first genetically confirmed case of OSTL1 with non-exon 2 mutations in COL2A1 in the Korean population.
Most COL2A1 mutations in STL1 are spread throughout the gene and are predictive of premature termination, suggesting that the phenotype usually results from a quantitative defect in type II collagen synthesis because of nonsense-mediated mRNA decay [11]. Two different COL2A1 transcripts resulting from alternative splicing of exon 2 have been reported [12]. NM_001844.4 is the longer transcript, and it contains a large cysteine-rich domain in the amino-propeptide encoded by exon 2, which is predominantly expressed in the vitreous body [13]. In contrast, the shorter transcript in which exon 2 is spliced out is predominantly expressed in adult cartilage. Therefore, mutations in exon 2 of COL2A1 have been considered to cause more damage in the eye than in other tissues.
However, we demonstrated that the OSTL1 is not confined to mutations in the alternative spliced exon 2. The first variant, c.2678dupC, is located in exon 40; it has been previously reported in one Caucasian patient with STL1 [11]. Although clinical information was not provided in that study, c.2678dupC could contribute to the ocular phenotype on the basis of our case report. The second variant, c.3327+1G>C, is located within the consensus splice site in intron 47. Richards et al. [14] also reported a COL2A1 splicing mutation involving intron 51 in an OSTL1 patient, suggesting that tissue-specific missplicing could be a mechanism.
Recent studies showed that preventive treatment can significantly reduce the risk of RRD [1516]; patients who did not receive prophylaxis had a 5-fold increased risk of RRD compared with those who received cryotherapy [16]. Therefore, high suspicion and genetic diagnosis for Stickler syndrome is important, given the emerging subgroup of OSTL1 with a high risk of RRD.
In conclusion, we identified two likely pathogenic variants of COL2A1, resulting from non-exon 2 mutations, which cause OSTL1. Clinicians should consider genetic diagnosis of OSTL1 in patients with vitreous anomaly to prevent blindness.
 XML Download
XML Download