

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor
Streptococcus tigurinus, a novel bacterial species, was first discovered by Zbinden et al. in 2012 [1]. Although S. tigurinus was reported to cause invasive infections, accurate identification of this organism requires genetic analysis [123456]. We report a patient with concurrent bacteremia, endocarditis, and spondylitis caused by S. tigurinus.
A 79-yr-old male presented with chills and back pain after treatment with acupuncture. A spinal magnetic resonance imaging and echocardiogram lead to the diagnosis of spondylitis and endocarditis. On admission, he was afebrile (36.5℃) with a blood pressure of 141/71 mm Hg. His leukocyte count was 14.7×109/L, with 88.6% segmented neutrophils. The serum C-reactive protein level was 8.95 mg/dL. Empirical antibiotic therapy of intravenous ceftriaxone, at a dose of 4 g/day, was initiated.
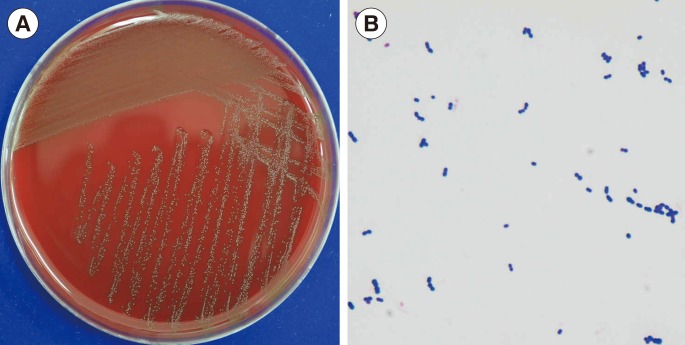
The patient underwent aortic valve replacement and a bone biopsy of the vertebral body. Whitish-gray pinpoint colonies with alpha-hemolysis were isolated from the bone culture, and Gram-staining revealed gram-positive cocci in chains (Fig. 1). The isolate was identified as Streptococcus mitis/Streptococcus oralis using Vitek II (bioMérieux, Marcy l'Étoile, France) and was sensitive to penicillin. The same microorganism was isolated from blood culture, and the valve tissue culture was negative. Therefore, the antibiotic therapy was changed to intravenous penicillin G, at a dose of 18 million IU/day.
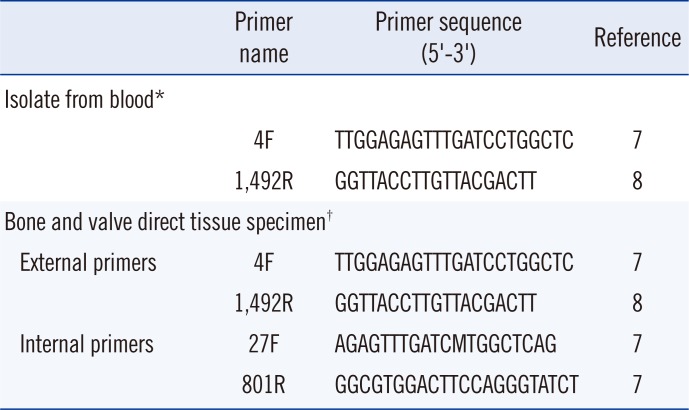
The bone and valve specimens and colonies from blood culture were analyzed by 16S rRNA gene sequencing. The 16S rRNA gene was amplified by standard methods according to CLSI guideline [7]. Primers were summarized in Table 1. The amplified sequences were compared with the NCBI Blast sequence database. The isolated 16S rRNA sequence was identical to the type strain AZ_3a of S. tigurinus (GenBank accession number, JN004270.1) with 99.8% of identity (1,463 of 1,456 bases). The most closely related species within the GenBank was S. sanguinis, with a sequence identity of 98.6%. Therefore, we identified this gram-positive coccus as S. tigurinus. The same results were obtained for bone and valve specimens, with a sequence identity of 100% (711/711 for bone and 683/683 for valve).
S. tigurinus was first isolated from patients presenting with infective endocarditis, spondylodiscitis, and meningitis [1]. It belongs to the Streptococcus mitis group and is closely related to Streptococcus mitis, Streptococcus pneumoniae, Streptococcus pseudopneumoniae, Streptococcus oralis, and Streptococcus infantis [1]. Colonies on sheep blood agar are circular, smooth, white to grayish, and alpha-hemolytic with a diameter of 0.5-1 mm after incubation at 37℃ under aerobic conditions for 24 hr [1].
Commercial testing systems such as Vitek II and matrix-assisted laser desorption ionization-time of flight mass spectrometry incorrectly identify S. tigurinus as S. mitis/S. oralis and S. pneumoniae, respectively [2]. An accurate species assignment as S. tigurinus is only possible using genetic analyses. A retrospective review of bacterial 16S rRNA sequences before recognition of S. tigurinus revealed 17 S. tigurinus sequences originally identified as S. mitis group [2].
S. tigurinus was reported to cause invasive infections such as endocarditis in both immunocompromised and immunocompetent patients [23456]. Whole-genome analysis of S. tigurinus revealed genes for known virulence factors [9]. Another study demonstrated that S. tigurinus shows an increased resistance to phagocytosis by macrophages and an increased ability to enter endothelial cells, with much lower ID90 than that of other endocarditis-causing strains [10]. Therefore, S. tigurinus is a clinically important pathogen that requires accurate identification by genetic analysis.
The presented case is the first reported patient with invasive S. tigurinus infection in Korea. The patient had concurrent bacteremia, endocarditis, and spondylitis due to S. tigurinus infection, whose site of origin was not known. S. tigurinus has been reported as a part of normal human oral flora [11]; therefore, bacteria from the oral cavity may enter the bloodstream and cause bacteremia, then endocarditis and spondylitis. However, in this case, the patient may have acquired bacteremia as a result of acupuncture. In this scenario, the patient may have developed spondylitis first, then bacteremia, and eventually endocarditis.
In antibiotic susceptibility testing, all strains were uniformly susceptible to penicillin and ampicillin. According to previous reports, the antibiotic susceptibility patterns of S. tigurinus are similar to those of other penicillin-susceptible viridans group streptococci [2312], and all patients were recovered after appropriate antimicrobial therapy [2]. Our patient was also fully recovered and discharged after six weeks of intravenous penicillin therapy.
In the present patient, the cardiac valve specimen was found to be culture-negative. A similar culture-negative case that required genetic analysis has been reported [5]. These findings further confirm the utility of 16S rRNA analysis in clinical microbiology.
 XML Download
XML Download