

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Aspergillus species are the most common causative agents of severe opportunistic fungal infections, especially in immunocompromised patients [1]. Although Aspergillus fumigatus remains the most common Aspergillus isolate recovered from clinical specimens, recent reports indicate the increasing prevalence of infections caused by other species of Aspergillus [2]. Accurate species identification is particularly important for determining the implications of resistance for patient management strategies, as some species show specific patterns of antifungal susceptibility [12]. However, misidentification is common when only macroscopic and microscopic morphologies are used [34]. A sequence-based identification method that uses the ribosomal internal transcribed spacer (ITS) region has been the gold standard for identifying various pathogenic fungi. However, for Aspergillus, ITS regions identify organisms only to the "species complex level" (that is, species that are morphologically or biochemically similar and otherwise indistinguishable by classical methods and/or ITS sequencing) [2]. By additional use of β-tubulin or calmodulin for fungal identification, several species have been revealed to be species complexes. They are formed by species that are almost indistinguishable by morphological methods, and hence, they have been designated cryptic species [2345]. Therefore, the International Society for Human and Animal Mycology-sponsored Aspergillus Working Group has recommended the use of a comparative sequence-based identification method that uses the ITS region for identification to the species complex level and a protein-encoding locus, such as the β-tubulin region, to identify Aspergillus species within complexes [5].
Amphotericin B (AMB) is the gold standard for treating a wide range of fungal infections [67]. Until recently, species identification was sufficient to guide AMB therapy, because Aspergillus terreus was the only organism with a consistently high AMB minimal inhibitory concentration (MIC) [6]. However, numerous new species have recently been identified by sequence-based analysis, and reduced susceptibility to AMB has also been found for cryptic species, such as A. lentulus, A. fumigatiaffinis, A. niveus, A. carneus, and A. calidoustus [27]. In addition, the frequent use of AMB and its lipid formulations continues to increase selection pressure, and therefore, monitoring for emerging AMB resistance in Aspergillus spp. is important [8].
To date, the species distribution determined by sequence-based identification and in vitro AMB susceptibility testing of clinical strains of Aspergillus has not been fully surveyed in Korea. In this study, we performed molecular identification and AMB susceptibility testing of 136 clinical isolates of Aspergillus species recovered at 11 university hospitals in Korea during a 3-month period. We compared Etests performed on Mueller-Hinton agar supplemented with glucose and methylene blue (Etest-MH) and on RPMI agar supplemented with glucose (Etest-RPG) with the CLSI broth microdilution method.
METHODS
1. Aspergillus isolates and species identification
A total of 136 clinical isolates of Aspergillus species were analyzed. All isolates were obtained from 11 university hospitals over a 3-month period from January 2013 to March 2013. Isolates were cultured from respiratory specimens (n=79), ear swabs (n=32), abscesses and wounds (n=17), body fluids (n=6), and tissues (n=2). All isolates were identified by sequencing of the ITS region of ribosomal DNA [9], followed by partial sequencing of the β-tubulin gene [10]. Gene sequences derived from the ITS and β-tubulin regions of all the Aspergillus isolates were compared with sequences available in GenBank by means of the BLAST program (http://blast.ncbi.nlm.nih.gov/Blast.cgi) to identify isolates to the species complex level (by using the ITS region) and to the species level within the complex (by using the β-tubulin region) [345]. The determined sequences were then compared. Results were considered acceptable if the homologies with other entries in the databases used for comparison were >99%.
2. Antifungal susceptibility testing
AMB MICs of each isolate were determined by the following three methods: CLSI M38-A2 broth microdilution assay, Etest-MH, and Etest-RPG. AMB MICs determined by the CLSI method were read after 48-hr incubation, with each MIC defined visually as the lowest concentration of drug that caused complete inhibition of growth (first clear well) relative to that of controls [11]. AMB Etests (bioMérieux SA, Marcy l'Etoile, France) were performed on the following two media as described previously [12]: (i) Mueller-Hinton agar supplemented with glucose (2%) and methylene blue (0.5 µg/mL) (Etest-MH) and (ii) RPMI 1,640 agar supplemented with 2% glucose (Etest-RPG). Etest AMB MICs on both media were read after 48-hr incubation at 35℃, with the MIC defined by the point of complete inhibition of visible growth, where the border of the elliptical inhibition zone intersected the scale of the strip edge. Two reference strains, Candida parapsilosis ATCC 22019 and Candida krusei ATCC 6258, were used as quality control isolates for each antifungal susceptibility test.
3. Analysis of results
The AMB MIC values were considered to be in essential agreement between the reference CLSI method and each Etest when the results were within two dilutions [1213]. Etest MICs were rounded to the next highest CLSI concentration to simplify comparisons, and the frequency of discrepancies among MIC endpoints of more than two dilutions (two wells) was used to calculate essential agreement. Since clinical breakpoints for AMB and all Aspergillus species have not officially been designated by the CLSI, we used the recently published epidemiological cutoff values (ECVs) for AMB, i.e., 2 µg/mL for the A. fumigatus, A. niger, A. flavus, and A. versicolor complexes and 4 µg/mL for the A. terreus complex, to classify the strains used in this study as wild type (WT) or non-wild type (non-WT) in resistance [813]. Categorical agreement was defined as the percentage of isolates classified by each Etest into the same category as that determined by the CLSI reference method. Discrepancies were considered to be "very major" when an isolate classified as non-WT (above the ECV) by the CLSI method was categorized as WT by an Etest and "major" when an isolate classified as WT by the CLSI method was classified as non-WT by an Etest [1213].
RESULTS
1. Molecular identification
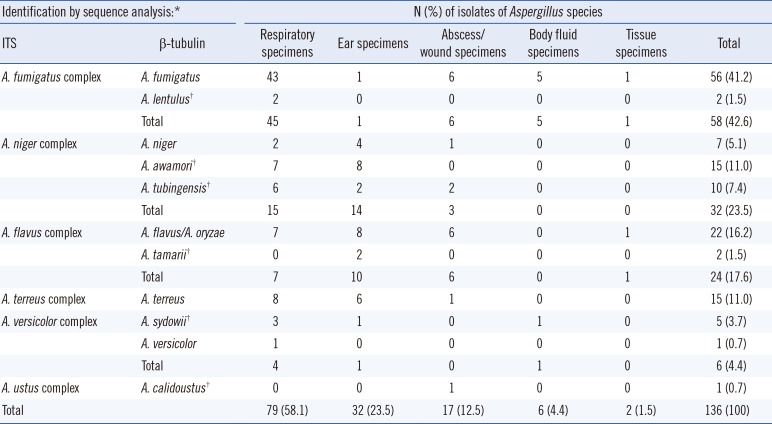
Table 1 shows the results of molecular identification for 136 isolates of Aspergillus. ITS sequencing identified the following six Aspergillus species complexes: A. fumigatus (42.6% of isolates), A. niger (23.5%), A. flavus (17.6%), A. terreus (11.0%), A. versicolor (4.4%), and A. ustus (0.7%). Of 79 respiratory isolates, 45 (57.0%) belonged to the A. fumigatus complex and 15 (19.0%) to the A. niger complex. Of 32 ear isolates, 14 (43.8%) belonged to the A. niger complex, 10 (31.2%) to the A. flavus complex, and 6 (18.8%) to the A. terreus complex. Cryptic species identifiable by β-tubulin sequencing accounted for 25.7% (35/136) of the isolates, with A. awamori (11.0%) as the most frequent species, followed by A. tubingensis (7.4%), A. sydowii (3.7%), A. lentulus (1.5%), A. tamarii (1.5%), and A. calidoustus (0.7%).
2. AMB MIC distribution by the CLSI method
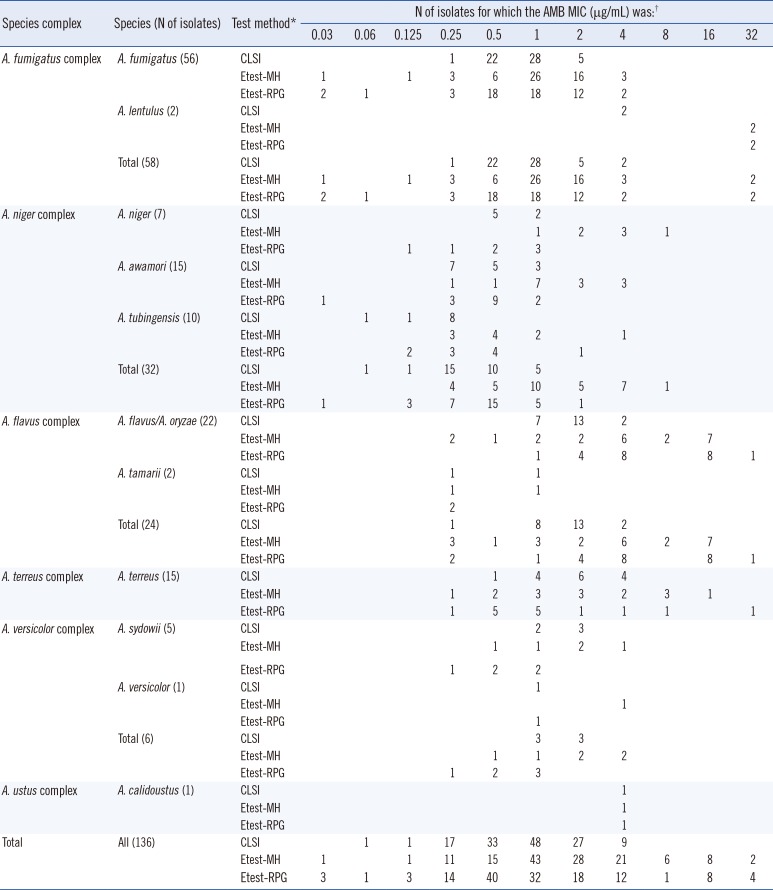
Table 2 shows the distribution of AMB MICs for the 136 isolates of Aspergillus determined by all three methods. The geometric mean values of AMB MICs (µg/mL) determined by the CLSI method were 0.8, 0.4, 1.5, 1.8, and 1.4 for the A. fumigatus, A. niger, A. flavus, A. terreus, and A. versicolor complexes, respectively. Of all 136 isolates, 36 (26.5%) had AMB MICs of ≥2 µg/mL by the CLSI method, including 7 A. fumigatus, 15 A. flavus, 10 A. terreus, 3 A. versicolor, and 1 A. ustus complex isolate. Two isolates of the A. fumigatus complex and one of the A. ustus complex, with an AMB MIC of 4 µg/mL, were identified as A. lentulus and A. calidoustus, respectively, by partial sequencing of β-tubulin. These A. lentulus and A. calidoustus isolates also had AMB MICs of >2 µg/mL by the two Etest methods. All 32 A. niger complex isolates, including A. niger, A. awamori, and A. tubingensis isolates, showed AMB MICs of ≤2 µg/mL by both the CLSI and Etest-RPG methods, but 25% (8/32) of the A. niger complex isolates showed AMB MICs of >2 µg/mL by the Etest-MH method. Two isolates of A. tamarii, which belongs to the A. flavus complex, showed AMB MICs of ≤1 µg/mL by all three methods. Of the three methods, Etest-RPG generated the broadest distribution of AMB MICs, with MICs ranging from 0.012 to 32 µg/mL, followed by Etest-MH (0.032 to 32 µg/mL) and then the CLSI method (0.06 to 4 µg/mL).
3. Comparison of AMB MIC results of the three methods
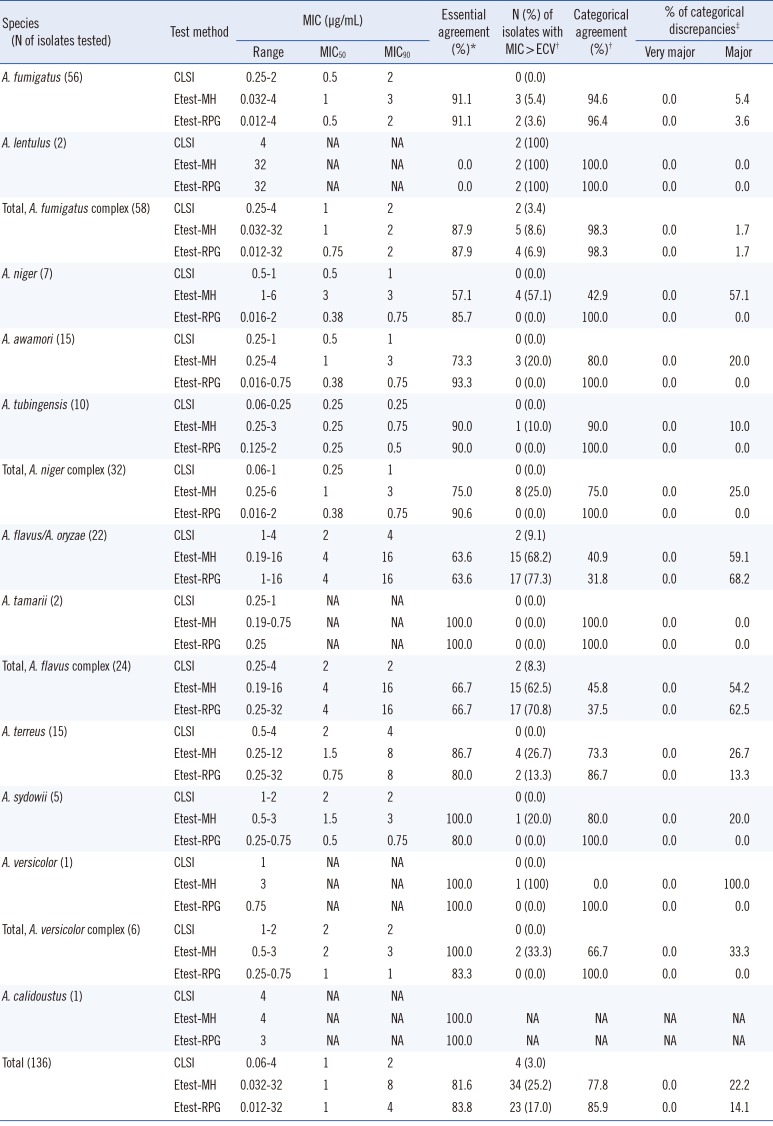
Of 136 total isolates, 3.0%, 25.2%, and 17.0% had AMB MICs that were greater than the ECVs by the CLSI method, Etest-MH, and Etest-RPG, respectively. For all 136 isolates, essential agreement with the CLSI method was 81.6% for Etest-MH and 83.8% for Etest-RPG. Categorical agreement with the CLSI method was 77.8% for Etest-MH (0% very major discrepancies and 22.2% major discrepancies) and 86.7% for Etest-RPG (0% very major discrepancies and 14.1% major discrepancies) (Table 3). AMB susceptibility testing by the two Etests showed > 98% of categorical agreements with the CLSI method for A. fumigatus complex but showed <50% of categorical agreements for A. flavus complex isolates (45.8% for Etest-MH and 37.5% for Etest-RPG). Categorical agreements of the Etest-MH results with those of the CLSI method were ≤75% for the A. niger, A. terreus, and A. versicolor complexes, while those of Etest-RPG were 100% for both the A. niger and A. versicolor complexes and 86.7% for the A. terreus complex.
DISCUSSION
At present, there is a lack of substantial research using molecular identification to characterize the distribution of Aspergillus species among Korean clinical isolates. Using sequence-based identification, the present study found that Aspergillus species other than A. fumigatus (non-fumigatus Aspergillus species) represented up to 60% of all Korean clinical isolates. The prevalence of A. fumigatus (41.2%) was lower than that reported in other studies (50-67%) [2], which may be explained in part by the larger proportion of ear isolates in the present study. A. fumigatus was present in 57.0% of the respiratory isolates, but non-fumigatus Aspergillus species made up 96.9% of ear isolates. Cryptic species, identifiable by β-tubulin sequencing only, accounted for 25.7% of the isolates, an incidence that is higher than that observed in other studies (10-14%) [2]. Notably, the present study revealed 15 isolates (11.0%) of A. awamori and 10 (7.4%) isolates of A. tubingensis, both of which were more common than A. niger. Until recently, A. awamori was treated as a synonym of A. niger, but the splitting of these two species was supported by amplified fragment length polymorphism (AFLP) analysis of whole genomes [14]. All 15 isolates of A. awamori in the present study showed 99-100% identity with sequences of the reference strains of A. awamori available in GenBank (accession number FN394674) [14].
Of all 136 isolates of Aspergillus, 36 (26.5%) had AMB MICs of ≥2 µg/mL by the CLSI method; these included 5 A. fumigatus, 2 A. lentulus, 15 A. flavus/A. oryzae, 10 A. terreus, 3 A. sydowii, and 1 A. calidoustus isolate. Among these species, A. lentulus and A. calidoustus are cryptic species, in which AMB resistance may be intrinsically present, as described previously [27]. All A. lentulus and A. calidoustus isolates had AMB MICs of >2 µg/mL by all three methods used in the present study. AMB MICs determined by the CLSI method for all 15 A. terreus isolates ranged from 0.5 to 4 µg/mL, and 10 (66.7%) isolates had AMB MICs of ≥2 µg/mL, similar to the results of previous reports [815]. However, both preclinical and clinical studies suggest that A. terreus is a poor target for AMB and can therefore reasonably be reported as AMB resistant without further antifungal testing [1617]. A. terreus represented 11.0% of all clinical isolates of Aspergillus species, an incidence higher than those in other reports (2.7-9.4%) [21819]. Overall, our results suggest that reduced AMB susceptibility is not uncommon among clinical isolates of Aspergillus in Korea and that the partial β-tubulin sequence is a promising locus for the accurate identification of Aspergillus species, especially cryptic species.
The CLSI method cannot detect AMB-resistant isolates of Candida species, and the Etest-MH method provides the best discrimination between AMB-resistant and -susceptible isolates of Candida [12]. To date, several studies have addressed the performance of the Etest method relative to the CLSI microdilution method for AMB susceptibility testing of Aspergillus species [2021222324]. However, in some previous studies, only a small number of isolates (5 or 10 isolates each of Aspergillus species) were tested [2021]. Higher levels of agreement of Etest-RPG with the CLSI method were found after 24 hr of incubation (81% within two dilutions) than after 48 hr of incubation (69% within two dilutions) for AMB [23]. However, we found that some isolates of Aspergillus species did not produce visible growth within 24 hr but had growth that was more obvious after 48 hr for Etests or the CLSI method, supporting the previous finding of the poor reproducibility of Etests, in particular, after 24 hr of incubation [21]. In a recent study, Colozza et al. [24] compared CLSI and Etest-RPG MICs for determinations of the Aspergillus species susceptibility to AMB of 103 isolates after 48 hr of incubation. They showed that essential agreement (within two dilutions) between the two methods was dependent on the species complex tested (100% for A. terreus, 97% for A. fumigatus, 77.8% for A. niger, and 58.3% for A. flavus). However, in previous studies, categorical agreements were not assessed because of the absence of clinical breakpoints or ECVs for Aspergillus species [2021222324]. We describe the first comparative evaluation of Etest-MH and Etest-RPG with the CLSI method for AMB susceptibility testing, with application of the recently published species-specific AMB ECVs [813].
When AMB MIC results of Etest-RPG and Etest-MH were compared to those produced by the CLSI method, essential agreement (within two dilutions) was found for 81.6% and 83.8% of all 136 isolates, respectively, and categorical agreements were found for 77.8% and 85.9%, respectively. There were no very major discrepancies in determining AMB sensitivity by either Etest. In this study, >90% of essential and categorical agreements for A. fumigatus were obtained between the CLSI method and both Etest methods, suggesting that either Etest may be useful for A. fumigatus. However, the categorical agreement of Etest-MH with the CLSI method was ≤75% for the A. niger, A. terreus, and A. versicolor complexes, while that of Etest-RPG was 100% for both the A. niger and A. versicolor complexes and 86.7% for the A. terreus complex. In particular, 25% of A. niger complex isolates were categorized as non-WT (MIC, >2 µg/mL) by Etest-MH, while none of these isolates were categorized as non-WT by the other two methods. Considering previous reports of no non-WT isolates of A. niger [8], these data suggest that Etest-MH may be inferior to Etest-RPG for AMB susceptibility testing of clinical isolates of Aspergillus.
Among five Aspergillus complex isolates, the poorest essential (66.7%) and categorical (37.5%) agreements between the CLSI method and the Etest-RPG methods were seen with the A. flavus complex isolates; the essential agreement results are consistent with previous findings [2024]. The reason for the poor agreement for isolates of A. flavus is completely unknown. However, in every instance, this low level of agreement was caused by A. flavus isolates for which the CLSI AMB MICs were low and the Etest MICs were much higher, indicating that the Etest may support better growth of A. flavus. A recent report indicated that AMB susceptibility testing with Etest-RPG represented the in vitro method that best correlated with the results of experimental infection with A. flavus and that a clinical isolate of A. flavus showing an MIC of ≥2 µg/mL may reasonably be considered resistant in vivo [25]. In the present study, Etest-RPG generated the broadest distribution of AMB MICs among the three methods, and it showed >98% of categorical agreement with the CLSI method for all Aspergillus complexes, with the exception of the A. terreus (86.7%) and A. flavus (37.5%) complexes. Colozza et al. [24] also inferred that Etest-RPG may be superior to the CLSI method for detecting AMB-resistant Aspergillus strains, perhaps because of the wider range of MIC distributions available on the Etest strip. Intrinsic AMB resistance has been recognized in A. terreus for many decades, but A. flavus has also been known to have decreased susceptibility to AMB [1]. Therefore, all of these data suggest that Etest-RPG may be a simple alternative for AMB susceptibility testing of isolates of Aspergillus species in the clinical laboratory, although the usefulness of Etest-RPG should be assessed further by comparison of clinical outcomes.
 XML Download
XML Download