

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Diabetes is characterized by chronic hyperglycemia and causes long-term complications like retinopathy, neuropathy, and nephropathy. It generally accelerates macro- and micro vascular changes. Because of lifestyle changes (i.e., eating more and exercising less), diabetes has become a global epidemic. Approximately 346 million people have been diagnosed with diabetes worldwide, and in the US, diabetes-related conditions account for 1 of every 7 dollars in the health care budget [1, 2]. Efficient and effective management is required to handle this epidemic. Portable glucose meters facilitate the short-term management of diabetes. Long-term prospective studies, notably the Diabetes Control and Complications Trial (DCCT), the UK prospective Diabetes Study Group (UKPDS), and the Epidemiology of Diabetes Interventions and Complications (EDIC) study, have provided definite evidence that diabetic complications are directly related to mean glycemia value, as measured by the HbA1c concentration [3-5]. This, along with successful standardization, has made the HbA1c concentration a valuable diagnostic tool for monitoring long-term glycemic control as well as defining specific treatment targets and decision limits. We review and discuss the analytical and clinical aspects as well as the remaining challenges of detecting the level of HbA1c.
ANALYTICAL ASPECTS
The relevance of the HbA1c concentration in diabetes management is well recognized by the diagnostic industry, and various commercial tests have been developed in this respect [6].
1. Methods
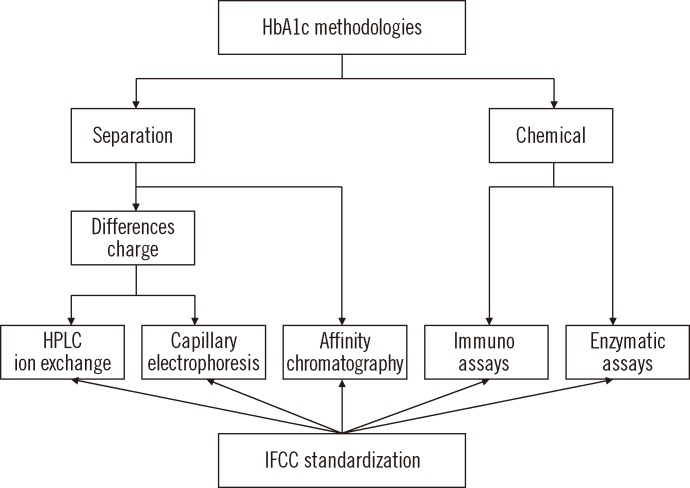
There are two major analytical concepts: one, based on the separation of Hb fractions and the other, based on chemical reactions (Fig. 1). Although different analytes are measured by these methods, assays can be standardized according to the Reference Measurement Procedure (RMP) of the International Federation of Clinical Chemistry (IFCC) [7, 8].
1) Separation methods
The fact that HbA1c and non-glycated Hb have different chemical properties allows for the separation of fractions and the quantification of HbA1c. This principle is applied in ion exchange chromatography (IEC), capillary electrophoresis (CE), and affinity chromatography (AC).
IEC: The pI of HbA1c and Hb differ by 0.02 units. This difference is sufficient to allow for the separation of HbA1c from non-glycated Hb via HPLC. With IEC, fetal Hb (HbF), minor fast Hb (HbA1a/b), and carbamylated Hb (HbCarb) as well as genetic variants (e.g., sickle cell Hb) can also be visualized [6].
CE: This method uses the charge difference between HbA1c and other Hb fractions. Separation is achieved via a high-voltage electrical field and electroosmotic flow [9].
AC: While non-glycated Hb runs freely through a column packed with boronic acid coated particles, glycated Hb molecules have an affinity to boronic acid, and HbA1c is retained on the column. This is the basis for separation. In addition to the N-terminal valine of the β-chain (HbA1c), glucose binds to approximately 15 other lysine residues in Hb. Altogether, these other glycated Hb account for approximately a half of all detected HbA1c molecules. As they are formed proportionally to HbA1c, calibration enables the results of the AC test to be expressed in terms of HbA1c [10].
2) Chemical methods
In chemical tests, HbA1c concentration is measured based on a specific chemical reaction to the glycated N-terminal valine of the β-chain. Total Hb concentration is measured in parallel with photometry. Two independent tests, HbA1c and total Hb tests, are therefore required to calculate the HbA1c concentration. This concept is applied in immunochemical and enzymatic assays.
Immunoassays (IA): In IA, an excess of anti-HbA1c antibodies is added to a hemolyzed sample. After binding to HbA1c, the excess antibodies agglutinate. The turbidity of the resulting immunocomplexes is measured photometrically using a turbidimeter or nephelometer. In parallel, the total Hb concentration is measured bichromatically in the pre-incubation phase [11].
Enzymatic assays: A protease cleaves the β-chain to liberate peptides. Peptides, usually dipeptides, react with fructosyl peptide oxidase, and the resulting hydrogen peroxide is used to quantify HbA1c. In parallel, the total Hb concentration is measured photometrically [12].
3) Strengths and weaknesses
The HbA1c concentration is a longitudinal parameter; patients are monitored over years or even decades. Therefore, a reliable test with highly reproducible results over a long period is required. For convenience, HbA1c measurements should preferably be available during the patient's visit to the physician or even be performed in front of the patient. Determining the HbA1c concentration is a high-volume test and therefore demands efficiency, a high throughput, robustness, and cost efficiency. The chosen method should also match the organizational structure i.e., it should be integrated into the general chemistry analyzer, a convenient stand-alone laboratory instrument, or as a point-of-care (POC) instrument in the doctor's office [6]. Priorities will differ according to the situation. Thus, the weight given to the strengths and weaknesses should be considered.
IEC meets the requirements of high throughput, quality, and robustness. Hb variants are seen, which can be regarded as a strength (detection of carriers and genetic counseling) or weakness (complications in routine laboratories and interference of HbA1c). A dedicated stand-alone instrument can also be a weakness. The same characteristics generally apply for CE. The runtime is considerably longer, which leads to better separation (no complications with variants). However, parallel capillaries must be operated to achieve high throughput. It can be challenging to achieve consistent results with all capillaries. If a robust column is required, AC can afford the same analytical quality as IEC, and variants are not seen. Chemical methods have the advantage that tests can simply be performed using general chemistry analyzers. However, the two independent tests required may negatively impact the analytical quality. Variants are not detected and do not interfere in the measurement. The analytical principles described apply to both laboratory and POC instruments. The strength of POC is its convenience of use, i.e., it requires no additional visit to the laboratory. A weakness is the questionable quality of the test that stems from the performance of the test itself or improper handling by non-laboratory staff.
4) Commercial versions
More than 100 commercial tests have been developed based on the five analytical principles described above. New assays, as well as modified versions of existing ones, continuously enter the market. It would be impossible to address all of them, and many are now obsolete. This review discusses only the general strengths and weaknesses. Up-to-date information on tests can be obtained from external quality assessment (EQA) or proficiency test (PT) programs.
2. Interferences
The most common interferences are Hb variants, elevated levels of HbF, and derivatives. Structural Hb variants have point mutations in the protein chains. Nine hundred variants have been identified, but 99% fall into four categories: S (high prevalence in black Africans and Americans, those of Mediterranean decent, and Indians), C (black Africans and Americans), E (South East Asian), and D (more equally spread over the globe). Synthetic variants arise from genetically determined changes in the capacity to synthesize Hb chains. In β-thalassemia, the production of β-chains is inhibited. When Hb molecules are assembled, β-chains are replaced by γ- or δ-chains, thereby elevating the levels of HbF and HbA2, which are normally very low. Derivatives (also called adducts) result from the posttranslational modification of Hb. Apart from HbA1c, the most common derivatives are HbCarb and pre-HbA1c (a Schiff base) [13].
The heterozygous forms of S, C, D, and E do not cause hemolytic diseases. As they all have a terminal β-valine, glycation is the same as that for HbA1c. The analytical interference of these Hbs is variant- and method-specific and is difficult to generalize [14]. The NGSP systematically evaluated most methods, and a periodically updated review can be found on the website [15]. As HbF has no β-chain and the γ-chain has a terminal glycine instead of a valine, HbF can only be glycated at lysine residues, resulting in a glycation rate of approximately one-third of that of HbA. With IA, the HbA1c concentration will decrease by 1%, and with AC, it will decrease by 0.7% for every 1% HbF. This interference becomes substantial at levels exceeding 10-15%. Both IEC and CE can generally separate HbF from HbA1c. The pI of HbCarb and pre-HbA1c roughly equals that of HbA1c. In older IEC methods, both HbCarb and pre-HbA1c would co-elute with HbA1c. In most instruments currently available in the market, they are separated well enough to prevent interference.
3. Standardization
1) Need for standardization
Different specificities and selectivities of routine methods lead to broad variation. However, optimal clinical use requires equivalence of results, regardless of the method used. Only then can the universal guidelines with uniform reference values and decision limits (and thus easy interpretation and comparability of scientific studies) be adhered to. Equivalence can be achieved through harmonization (calibration of routine methods against an arbitrarily designated comparison method) or standardization (calibration against a reference measurement procedure of higher metrological order) [16].
2) Harmonization
The well-recognized need for equivalence initiated national harmonization efforts. In the US, the arbitrarily chosen method was the method used as the anchor in the DCCT Study. The nationwide program with international affiliations was, and still is, organized by the NGSP [17]. Similar programs resulted in harmonization in Japan (Japan Diabetes Society/Japanese Society for Clinical Chemistry) and Sweden (Mono-S) [18, 19]. Unfortunately, the methods of these harmonization efforts yielded variable results.
3) Standardization
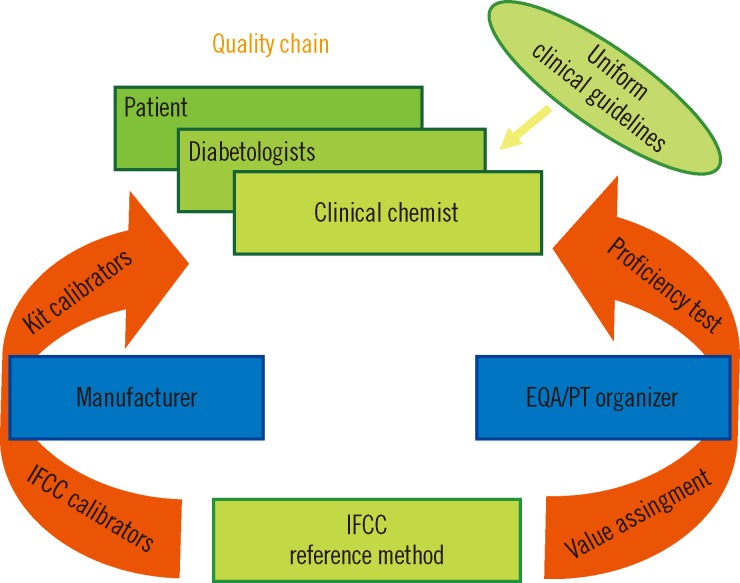
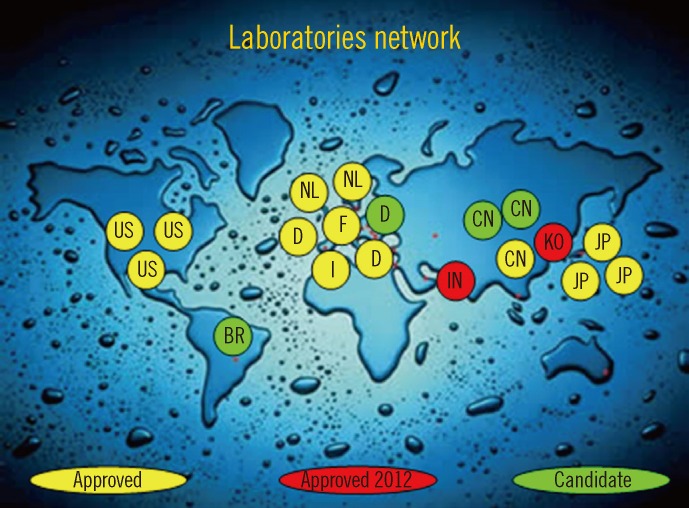
The aforementioned situation created confusion. The IFCC therefore developed a reference measurement procedure of higher metrological order (IFCC-RMP) to achieve worldwide standardization [7, 19]. The IFCC-RMP is based on the concept of metrological traceability. Pure HbA1c and HbA0 are mixed to calibrate the IFCC-RMP. Hb-containing washed and lysed erythrocytes are cleaved with endoproteinase, and the resulting hexapeptides are measured with either HPLC-CE or HPLC-electrospray mass spectrometry. With the IFCC-RMP, values are assigned to whole blood panels that serve as calibrators for manufacturers. In this way, the complete quality chain from IFCC-RMP to patient is created (Fig. 2). The IFCC-RMP is embedded in a global network of reference laboratories in Europe, Asia, and the US [20] (Fig. 3).
4) Consensus statement
The ultimate aim of the IFCC is the global standardization of all routine methods. The HbA1c concentration of patients should be reported in the International System (SI) of units. Unfortunately, universal reporting will unlikely be achieved; there was, and still is, resistance against a change of units [21]. To solve this dilemma, the IFCC and the major diabetes organizations-the International Diabetes Federation (IDF), the European Association for the Study of Diabetes (EASD), and the American Diabetes Association (ADA)-agreed on a consensus statement [22]. The major statements are: 1) the IFCC-RMP for HbA1c represents the only valid anchor to implement standardization of the measurement; 2) HbA1c results are to be reported by clinical laboratories worldwide in SI units (i.e., mmol/mol) and derived NGSP/DCCT units (%); and 3) editors are strongly recommended to report HbA1c concentrations in both units. However, reporting patient results in both units is unpractical, and the HbA1c concentration is often reported in only one set of units.
5) Master equations for conversion IFCC/NGSP
The master equations for converting IFCC units into NGSP units (NGSP%=0.0915×IFCC mmol/mol+2.15) and vice versa (IFCC mmol/mol=10.93 NGSP%-23.5) are established and monitored by the IFCC and NGSP networks [20].
In summary, full (all routine methods are calibrated against the IFCC-RMP) and partial standardization of reported patient results (IFCC and NGSP units) have been established.
4. Quality management
The HbA1c concentration is the ultimate longitudinal parameter; therapy depends on serial HbA1c measurements over a period of years or decades. Therefore, considerable attention should be given to quality management.
1) Pre-analytical considerations
Unlike glucose samples, HbA1c samples can be easily collected and stored. Blood can be taken at any time without patient precautions. Blood obtained by venipuncture or finger-stick capillary is suitable. Unless otherwise specified by the manufacturer, the anticoagulant should be EDTA. Sample stability is method specific. HPLC methods are most sensitive to aging effects. Some POC tests cannot measure even slightly hemolyzed specimens. Blood is generally stable for up to 1 week at 2-8℃. Blood stored below -70℃ is stable for at least 1 yr. Storage at -20℃ has adverse effects and should be avoided [23]. Some manufacturers have developed method-specific collection systems to facilitate field-collection (e.g., filter paper and micro-cups with lysing buffer). These systems should only be used if validated in comparison with standard collection [21].
2) Post-analytical considerations
Results below the lower limit of the reference interval should be confirmed with repeated testing. If confirmed, the clinician should be informed about the possibility of variant or shortened erythrocyte survival. Samples with extremely high results (>140 mmol/mol or >15%) and those for which the results do not match the clinical picture should be re-assayed. Repeated testing with a different analytical method can help detect the reason for unexpected patient- or method-related results.
3) Quality system
In qualified laboratories, a quality system consisting of three basic principles is in place: accreditation to the International Organization for Standardization (ISO) 15189, internal QC, and EQA. For internal control, two control samples (with low and high HbA1c concentrations) should be assayed in every analytical run. Frozen whole-blood aliquots stored below -70℃ and lyophilized hemolysates with no or known matrix effects are suitable [21]. Participation in an EQA or PT program provides valuable external information for managing the quality of the HbA1c test. Bias is derived from the EQA target set with the IFCC-RMP, performance is compared with other laboratories using the same method, and EQA reports provide an up-to-date review of available methods and their performances.
4) Performance goals
The reliability of HbA1c measurement depends on bias (related to proper calibration) and precision (related to the reproducibility of the method). Quality goals can be derived from biological variation, clinical needs, or the state of the art. For HbA1c, a generally accepted rule of thumb is that clinicians interpret a difference of 5 mmol/mol (0.5%) between successive patient samples as a significant change in glycemic control [24]. Therefore, the intralaboratory CV (derived from the lab's internal QC records) should be <3% (<2% NGSP units). The overall interlaboratory CV (derived from the EQA review) should be <5% (<3.5% NGSP units) or <4.5% (<3% NGSP units) within one method [21]. The difference in performance goals is derived from the unspecificity of the NGSP reference method [25].
5) Quality POC testing
The quality concept used in laboratories is not usually applied to POC testing settings. Careful reading of the instructions, checking if the manufacturer warrants traceability of results to the IFCC-RMP, and periodic exchange of samples with a qualified laboratory, all contribute to the quality of the test. Participation in an EQA program is strongly advised. In situations where no EQA is available, a professional organization or the government should carry out EQA.
CLINICAL ASPECTS
1. Clinical use
1) Monitoring
The HbA1c concentration is widely used for the routine monitoring of long-term glycemic status in both type I and type II diabetes patients. HbA1c is the index of mean glycemia and as such, documents the degree of glycemic control, response to therapy, and risk for developing or worsening diabetes complications [3, 26].
2) Diagnosis
Considering improved standardization of the test and recent data demonstrating the relation with retinopathy, an international expert committee recommended using the HbA1c concentration for diagnosing diabetes. This view has been adopted in many countries including the US, Japan, and the United Kingdom. However, application in daily practice varies from replacing the glucose tolerance test and/or fasting plasma glucose to using HbA1c measurements in parallel to these tests [27-29]. The WHO recommends that "HbA1c can be used as a diagnostic test for diabetes providing that stringent quality assurance tests are in place and assays are standardized to criteria aligned to the international reference values, and there are no conditions present that preclude its accurate measurement." These conditions include pregnancy, suspected type I diabetes, a short duration of diabetes symptoms, acute illnesses, receiving medication that may cause a rapid increase in the glucose level, pancreatic damage, hemoglobinopathies, anemia, renal failure, and HIV infection [30].
3) Pregnancy
A specific application is the use of HbA1c measurements during pregnancy in patients with diabetes to determine the minimal perinatal risk for the mother and maximum health of the fetus. Stringent control prior to and during pregnancy decreases the risk of congenital malformations, overweight infants, as well as complications of pregnancy and delivery related to poorly managed glycemic control [31].
4) Assessment quality diabetes care
Health care authorities indirectly use HbA1c measurements when assessing the quality of diabetes care. The (frequency of) use by health care providers and the mean value or proportion of patients below a specific target is monitored [32].
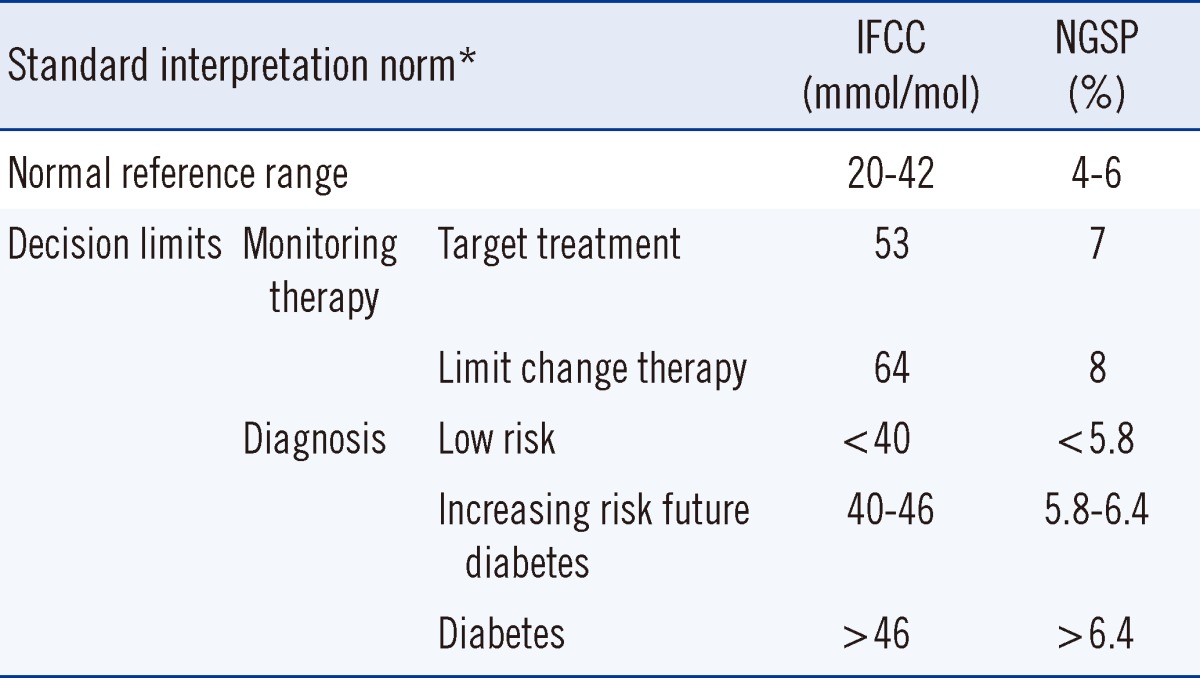
2. Standard interpretation norms
The normal reference range and clinical decision limits for IFCC/NGSP-standardized HbA1c concentration are summarized in Table 1. The normal reference range is derived from the landmark DCCT Study [3]. The general target for treatment of diabetes patients is 53 mmol/mol (7%) with the recommendation to strengthen therapy when the level of HbA1c exceeds 64 mmol/mol (8%) [26]. The HbA1c concentration represents a continuum: values <40 mmol/mol (5.8%) indicate a low risk for diabetes, whereas those >46 mmol/mol (6.4%) indicate the presence of diabetes. HbA1c concentrations of 40-46 mmol/mol (5.8-6.4%) are associated with an increasing risk of diabetes [26]. Serial measurements may improve the HbA1c concentrations in type I patients, but there is no consensus on the optimal frequency of HbA1c testing [33]. The frequency depends on the clinical condition of the patients. In stable, well-controlled situations, the frequency can be lower than that for patients with poor control. The ADA recommends at least two tests a year for patients who meet treatment goals (and who have stable glycemic control), and quarterly tests in patients whose therapy has changed or who do not meet glycemic goals. In addition, all patients with diabetes who are admitted to a hospital should have their HbA1c concentrations measured if the test results of the previous 2-3 months are unavailable [27].
3. Interpretational considerations
Although standard interpretation norms are applicable, any result should be interpreted with caution because of uncertainty. Additionally, specific clinical conditions and individualized targets for therapy should be considered.
1) Uncertainty
The uncertainty of laboratory test results is often underestimated, especially by clinicians. Patient-related uncertainty stems from non-glucose-related biological variation. For HbA1c values, the major factor is erythrocyte lifespan. In normal individuals, erythrocytes survive for approximately 120 days. An HbA1c value of 43 mmol/mol (6.1%) implies a high risk for diabetes in cases where the erythrocytes have a relatively short lifespan and a low risk for diabetes in cases where erythrocytes have a relatively long lifespan. Test-related uncertainty stems from analytical errors in the test: systematic bias due to non-ideal calibration and random bias because of imprecision [6]. Interpretation uncertainty is the sum of patient- and test-related uncertainty. Because of the small margins in clinical decision limits, uncertainty should always be taken into account, especially when the HbA1c concentration is used for diagnosis.
2) Specific clinical conditions
The major advantage of HbA1c is the lack of impact of fluctuating glucose after meals and with illness. However, several conditions should be considered. In clinical conditions where the erythrocyte lifespan is substantially shorter (e.g., renal anemia with use of erythropoietin, chronic and hemolytic anemia, acute blood loss, and recent transfusion), results will show a false, low-level HbA1c. Liver disease, dialysis, and chronic malaria may also cause a false, low-level HbA1c. Iron deficiency anemia may cause a false, high-level HbA1c because of (assumed) altered glycation rates [14, 21]. The impact of age and race is currently under discussion. Some studies show that the HbA1c concentration increases by approximately 1 mmol/mol (0.1%) per decade [34]. Other studies suggest that the HbA1c concentration is higher in US African Americans and Hispanic populations than in Caucasians, but there are no definite conclusions. It is also unclear whether this would have clinical significance [21]. Although it is assumed that reference ranges and decision limits for Asians are similar to those for Caucasians, this has not been confirmed in reliable epidemiological studies in Indo-Asian and Sino-Asian populations.
3) Individualized targets
Targets are derived from the balance of minimum long-term complications, minimum risk of hypoglycemia, and quality of life. The longer is the life expectancy, the greater is the chance of long-term complications. More stringent targets for therapy will therefore be beneficial. If the life expectancy is low, the quality of life should be the priority, and overly strict regimens should be avoided. Lower targets can also be considered for patients with a short duration of diabetes and the absence of cardiovascular disease, and in type II diabetes patients on a diet. Higher targets are indicated for individuals with advanced vascular complications or a high frequency of hypoglycemia, as well as for children and adolescents [27]. Efforts to achieve an extremely low HbA1c concentration are controversial; apart from the increased frequency of hypoglycemic episodes, clinical conditions such as macrovascular diseases do not decrease or even increase with a lower HbA1c concentration [21].
4. Present and future
Since the landmark clinical trials (DCCT, UKPDS) clearly demonstrated the relationship between glycemic control, HbA1c, and diabetic complications, the test has greatly improved, thanks to the IFCC/NGSP standardization and the ongoing efforts of the diagnostic industry. The HbA1c concentration is now a reliable test and indispensable tool in both the routine management and diagnosis of diabetes. However, global availability and accessibility of adequate assays, with traceability to the IFCC-RMP have not yet been achieved, especially in developing countries. The IFCC-RMP has been adopted as the only valid anchor for standardization, but the HbA1c concentration is still reported in different units; universal reporting therefore remains a challenge. Although the HbA1c concentration is being more frequently used for diagnosis, the degree to which biological variation limits its application needs to be resolved. Further refined reference values and clinical decision limits related to age, ethnicity, and specific patient groups need to be developed. The use of POC instruments for diagnosis is controversial. Only a few devices meet the acceptable performance criteria and how the quality of the test will work in the hands of non-professionals is questionable [35]. No objective external information is available as long as participation in EQA programs is not mandatory. Improvement of the tests and the introduction of a quality concept to warrant acceptable performance by non-laboratory staff is a challenge. Although a higher number of and better tools for the management of diabetes are now available, there is still much to be learned by clinicians, patients, and laboratory technicians, i.e., how to use these tools and how HbA1c measurements can be utilized to achieve better patient care.
 XML Download
XML Download