

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
More than 400,000 neonates are born each year in Korea [1], and a fraction of them are born under the tertiary hospital setting. In a tertiary hospital, resident physicians as well as staff are in charge of the management of vaginal deliveries, especially in cases of low-risk pregnancies. Recently in Korea, based on a minor opinion, there was a social concern that deliveries done by resident physicians may be associated with the sub-optimal management in obstetrical service. On the other hand, in other developed countries such Canada and Japan, vaginal deliveries have been managed not only by obstetricians but also by family physicians and midwives [2,3].
The associations between maternal complications and the experiences of obstetricians have also been reported so far. Recently, it has been demonstrated that women, taken cared by obstetricians with a low volume of deliveries have greater maternal complications such as genital tract laceration or hemorrhage when compared with the cases treated by obstetricians, who have handled a high volume of deliveries [4]. In addition, a previous study found that the academic affiliation and obstetric volume of the delivering hospital were important predictors of clinical outcomes such as Cesarean delivery rate, episiotomy and laceration [5]. However, these studies mainly assessed the maternal complication and neonatal outcomes were not appraised. Meanwhile, the effect of hospital technology upon perinatal mortality has been demonstrated to be important for high-risk infants [6]. However, based on a recent study, no difference was observed in perinatal outcomes including Apgar score below 7 at 5 minutes, metabolic acidosis and transfer to neonatal intensive care unit (NICU) among the level of care centers in low-risk pregnancies according to the hospital volume or level [7].
With respect to the aforementioned backgrounds, since we could not find the currently available data on the comparison of neonatal outcomes between deliveries provided by staff and those by resident physicians in Korea, we decided to determine whether the neonatal outcomes and intrapartum events differ in the case of women with low-risk pregnancies, who obtain obstetrical procedure during their deliveries from resident physicians as compared with the procedures provided by staff.
Materials and methods
There were 15,530 deliveries in our institution during the study period, from January 2003 to March 2010. We excluded the cases with following pregnancy: multiple pregnancies, pregnancies complicated due to presence of maternal medical diseases including diabetes, hypertension, thyroid disease, malignancies and rheumatoid diseases, fetal congenital abnormality, gestational age of less than 37 weeks at delivery and deliveries by Cesarean section due to any cause. Accordingly, we excluded 7,251 pregnancies with multiple pregnancies, maternal medical diseases, congenital anomalies and gestational age of less than 37 weeks at delivery and 3,272 deliveries by Cesarean section. Finally, we conducted a retrospective cohort study by including 5,007 singleton full term vaginal deliveries.
We divided our study population into two groups according to the obstetricians recorded in the delivery notes; one group delivered by staff and the other group delivered by resident physician. We also divided these two groups into the subgroups based on delivery conducted by faculty versus by fellow and the subgroups delivered by junior versus senior resident, respectively. We always record the obstetricians who delivered the neonate and provided the obstetrical procedures on the delivery notes. The staff was defined as a doctor who has been certified as an obstetrics and gynecologic specialist from Korean Society of Obstetrics and Gynecology, and was consisted of faculty and fellow. The resident physician was defined as a doctor who was in residency training in obstetrics and gynecology at Samsung Medical Center and consisted of senior and junior. The senior resident physician was defined as third or fourth grade resident physician and the junior was defined as first or second grade physician. According to our own protocol at delivery floor, deliveries by junior resident physicians were supervised and attended by senior resident physicians.
We investigated maternal demographic characteristics including age, parity, and body mass index (BMI). Maternal BMI was calculated using maternal weight and height (at the time of admission for delivery) through medical records. Gestational age was calculated using the last menstrual day and was confirmed by ultrasound assessment in the first trimester. Neonatal outcomes, including birth weight, rate of large for gestational age (LGA), gender, Apgar score, admission to NICU and umbilical arterial cord pH after birth were also reviewed. We also assessed intrapartum events which were defined as shoulder dystocia and vacuum delivery. Shoulder dystocia was defined as a delivery that requires additional obstetric maneuvers such as suprapubic pressure or the McRoberts maneuver to release the shoulders after gentle downward traction has failed [8]. We compared baseline maternal characteristics, neonatal outcomes and the rate of intrapartum events according to study groups. The Pearson chi-squared test and Fisher's exact test were used for categorical variables, and the Student's t-test was used for continuous variables. All the analyses were performed by using SPSS ver. 19.0 (IBM Corp., Armonk, NY, USA).
Results
From the total study population, 2,631 deliveries (52.5%) were conducted by staffs and 2,376 deliveries (47.5%) were conducted by resident physicians. Typically, 1,768 deliveries (67.2%) conducted by staff were provided by faculty and 863 deliveries (32.8%) were provided by fellows. Meanwhile, senior residents provided 881 deliveries (37.1%) of resident physicians and junior resident physicians provided 1,495 deliveries (62.9%).
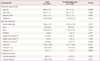
Comparisons of maternal characteristics, neonatal outcomes and the rate of intrapartum events between deliveries provided by staff and resident physicians are shown in Table 1. Based on the comparative analysis of the deliveries conducted by resident physicians, the proportion of nulliparity (59.9% vs. 50.3%, P < 0.001) and LGA (5.9% vs. 4.0%, P = 0.003) were higher in the deliveries by staff. However, there was no significant difference in neonatal outcomes including Apgar score, admission to the NICU and umbilical arterial pH (at birth) between two groups. In contrast, the rate of shoulder dystocia and vacuum delivery were significantly different between two groups. The deliveries provided by staff showed a higher rate of shoulder dystocia (1.4% vs. 0.8% P = 0.047) and showed a higher rate of vacuum delivery (13.8% vs. 4.7%, P < 0.001). There was no neonatal death from the total population included.
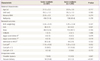
Table 2 shows maternal characteristics, neonatal outcomes and rate of shoulder dystocia and vacuum delivery between deliveries provided by faculty and fellows. Similar to the results shown Table 1, there was no significant difference in neonatal outcomes between two subgroups but women whose labors were attended by fellows were younger than those were attended by faculty (P = 0.001). Although, there was no difference in the rate of shoulder dystocia between two subgroups, the rate of vacuum delivery was higher in deliveries provided by faculty when compared to the deliveries provided by fellows (14.9% vs. 11.6%, P = 0.022).
Table 3 shows the comparisons between deliveries provided by senior and junior resident physicians. Interestingly, the mean value of umbilical arterial pH in deliveries provided by senior resident physicians tends to be lower than junior group (P = 0.052). Also, the rate of Apgar score below 7 at 5 minutes in deliveries provided by senior resident physicians was higher than the junior group (0.5% vs. 0.0%, P = 0.019). There was no difference in the rate of shoulder dystocia between two subgroups, however the rate of vacuum delivery was higher in deliveries provided by senior resident physicians than the junior group (10.4% vs.1.3%, P < 0.001).
Discussion
To the best of our knowledge, this is the first study about the comparisons of neonatal outcomes and the rate intrapartum events according to the grades of obstetricians in Korea. Our study clearly demonstrates that there exists no difference in the neonatal outcomes including Apgar score, admission to the NICU and umbilical arterial pH irrespective of whether staff or resident physicians perform delivery in women with low-risk pregnancies. Interestingly, obstetricians with more experiences showed the higher rate of intrapartum events including shoulder dystocia and vacuum delivery than the less experienced obstetricians. Our study result implicates that obstetricians with more experiences might tend to participate in difficult labors and prefer applying vacuum than the obstetricians with fewer experiences.
This study also demonstrates that women whose neonates were delivered by staff had a higher rate of nulliparity and LGA than in the deliveries conducted by resident physicians, and women whose neonates were delivered by fellows were younger than the cases handled by faculty. Demographic differences among patients according to the medical provider type have been represented in other studies. Patients of resident physicians were younger, non-white and more likely to be reimbursed by Medicaid [9,10]. The ethnicity and insurance status of our study population was homogenous; therefore, we did not investigate these factors. The difference in the rate of nulliparity may be derived from the issue that staffs offer the opportunities to resident physicians to provide obstetrical procedures in the cases of easier labors. Despite of excluding diabetes in this study, a difference in the rate of LGA between two groups was found and this may be associated with the increase in the rate of shoulder dystocia and vacuum delivery in the staff group. In fact, when we reanalyze our study population after the exclusion of the LGA, we found that the rate of shoulder dystocia was not different between deliveries conducted staff and resident physicians (1.0% vs. 0.7%, P = 0.235) but the rate of vacuum delivery remained different between two groups.
In addition, subgroup analysis also showed that women whose neonates were delivered by faculty or senior resident physicians had a higher rate of vacuum delivery than in the cases handled by fellows or junior resident physicians. This finding could suggest that obstetricians with more experiences tended to participate in difficult labors and choose to apply vacuum rather than perform Cesarean section for failure to progress. Interestingly, the rate of Apgar score below 7 at 5 minutes was higher and the mean value of umbilical arterial pH tended to be lower in the senior group than in the junior group. Though the reason for such a result is not clear, it is assumed to be derived from the fact that senior resident physicians usually attended difficult labors during nighttime. However, the differences in Apgar score or umbilical arterial pH may not be associated with an increase in the rate of NICU admission. Meanwhile, it is worth mentioning that most deliveries by junior residents were performed under the supervision of senior resident physicians as described in material and method.
There are several limitations in our study. First, we have not compared the rates of maternal complications such as postpartum hemorrhage and third-or fourth degree laceration. Also we have not compared the rates of neonatal morbidities such as brachial plexus palsy or cephalohematoma associated with difficult labors. The reasons we could not analyze these points were maternal complications seem to be difficult to assess objectively and the neonatal morbidities were rare in our study populations. In addition, these outcomes lie beyond the scope of our investigation, we did not investigate these points. Second, we have obtained umbilical cord gases incompletely (47.4% from the total population) as we changed the policy to analyze cord blood gases from all the deliveries from the middle of the study period. Third, although the difference in the indication or rate of Cesarean delivery between deliveries conducted by staff and resident physicians may be important, we could not analyze it. Because, almost of decisions on the mode of delivery including emergent Cesarean section due to dystocia was made by staff physicians and almost of Cesarean deliveries were performed by staff physicians. Lastly, the total study population was not powered enough to assess the neonatal death, which did not occur in our study population, restricting the statistical analysis between groups. However, it may be an obligate phenomenon since the subjects of this study comprised of full term vaginal delivery in the case of low-risk pregnancies excluding multiple pregnancies, maternal medical diseases, and fetal congenital abnormality.
In conclusion, there was no significant difference in neonatal outcomes between the two groups; staff versus resident physicians in full term vaginal deliveries in low-risk pregnant women. Therefore, the role of resident physicians on vaginal deliveries in low-risk pregnancies must continue to be emphasized in Korea.

 XML Download
XML Download