

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
During root canal instrumentation, procedural mishaps such as ledges, zips, strips, instrument separations, and perforations may occur. The development of dentinal defects may also be caused by root canal instrumentation [1]. These dentinal defects have been associated with a decreased outcome in an apical microsurgery model [2] and were proposed to contribute to vertical root fractures.
The root sectioning methodology has been repeatedly used to evaluate the presence of dentinal defects after root canal instrumentation [3], filling [4], and re-treatment [5]. In these studies, the experimental roots are sectioned, and pictures are taken to assess the creation of dentinal defects after root canal instrumentation [6]. A recent study, using the root sectioning methodology, has concluded that under light-emitting diode (LED) transillumination, uninstrumented roots presented defects that could not be visualized with magnification alone [7]. Root sectioning methodology is dependent on a negative control group presenting no defects that is compared with the experimental groups. Therefore, it is proposed that an improved model with minimal dentinal defects is needed.
Rose and Svec [8], in an in situ pig jaw model, suggested that when teeth are maintained in their original environment, root canal instrumentation does not create dentinal cracks. Arias et al. [9] used a cadaver model and found a similar number of defects in instrumented and uninstrumented roots. Different studies have also questioned the creation of dentinal defects by root canal instrumentation [1011]. It has been suggested that tooth sectioning might create defects that are not related to the root canal procedures [11]. In addition, unknown condition of the donated tooth, the lack of control of the donor's age, and specimen storage might have led previous studies to inaccurate conclusions [12]. We hypothesize that teeth removed with minimal extraction forces and processed promptly will exhibit fewer dentinal cracks than teeth having unknown extraction and storage conditions.
Therefore, the aim of the present study was to evaluate the presence of dentinal defects of uninstrumented, freshly extracted, periodontally involved roots compared with those of extracted roots with unknown history.
MATERIALS AND METHODS
The study samples were 18 roots collected from the Graduate Periodontology Clinic of the University of North Carolina at Chapel Hill, over 6 consecutive months that started in November 2015. Informed written signed consent was acquired from all participants according to the Declaration of Helsinki, and exempt status was approved by the Institutional Review Board Office of Human Research Ethics at the University of North Carolina at Chapel Hill (#15-1246). These roots served as the experimental samples (group 1), and the control (group 2) consisted of 18 matched similar root types obtained from an anonymous tooth collection, as was done in previous dentinal defect studies [710].
The inclusion criteria in group 1 were teeth scheduled for extraction due to severe chronic periodontitis. The teeth in group 1 were obtained from patients older than 18 years and presenting mobility Class II (horizontal mobility of more than 1 mm) or III (horizontal mobility of more than 1 mm and vertical mobility) [13]. The age and sex of patient, and the mobility of the teeth were recorded. Only roots presenting with mature apices and no signs of intraradicular treatment were included. After extraction, the teeth were immediately immersed in saline and kept in a humid environment during all procedures. Teeth in group 2 were the teeth that were extracted during the past 3 years for reasons not related to this study. They were rinsed with 0.5% NaOCl and then stored in saline. Teeth in group 2 also had mature apices and no signs of endodontic treatment or intraradicular posts. Each tooth was selected in order to match with the tooth type collected in group 1. In addition, root length and curvature was selected to be as similar as possible with a correspondent tooth in group 1. The conditions under which these control teeth were extracted, or the patient's age and sex were not known.
The sectioning of the roots was done using a low-speed saw (Isomet 1000, Buehler, Lake Bluff, IL, USA) under water irrigation. The slices were obtained at distances of 3, 6, and 9 mm from the apex. Pictures were then taken with a camera (Nikon D5100, Nikon Corporation, Tokyo, Japan) attached to a dental operating microscope (Global G6, Global Surgical Corporation, St. Louis, MO, USA) under × 19.2 magnification for the 3 and 6 mm slices. Pictures at the 9 mm slices were taken at × 12.8 magnification to allow the entire root cross-section to be viewed. An LED transilluminator (TransCure-T, Kinectic Instruments Corporation, Bethel, CT, USA) was used in the 4 different sides (mesial, distal, buccal, and lingual), resulting in 4 pictures for each section. The specimens were kept out of saline for less than 60 seconds during the imaging to avoid dehydration. Group 1 specimens were sectioned and photographed within 1 hour of extraction. Both groups were sliced and photographed following the same steps.
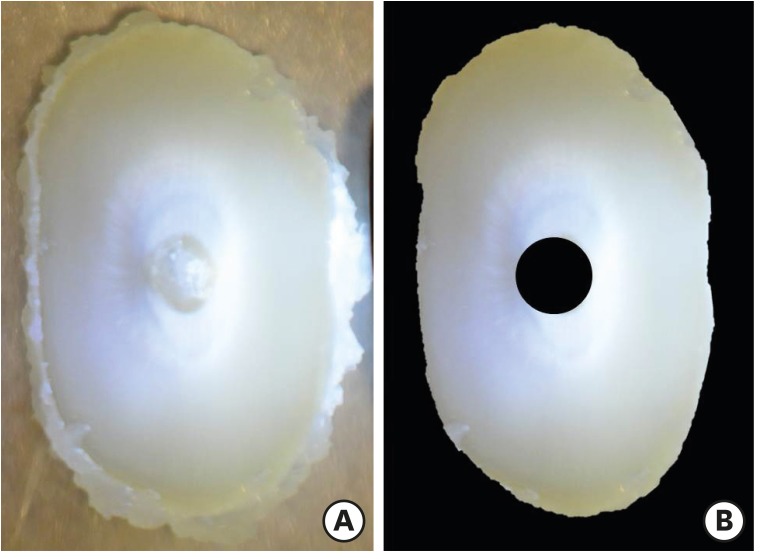
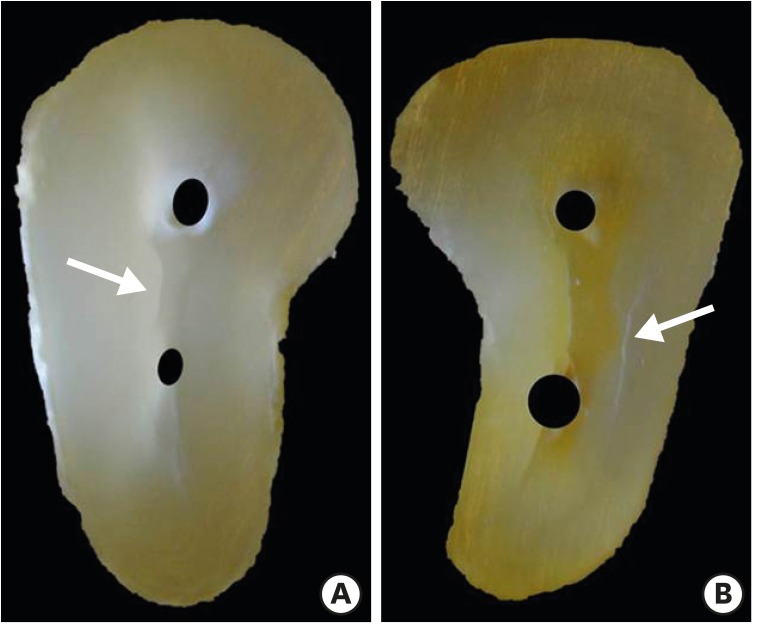
In order to mask the evaluators from the source of the specimen (since group 1 had fresh pulp and periodontal tissue remnants still attached), the root canal space on the pictures was masked with black circles, and the remnants of the periodontal ligament were covered (Figure 1). Two evaluators, endodontic specialists with clinical and research experience, assessed the roots for dentinal defects. In cases of disagreement, they discussed their decision until a consensus was reached. The evaluators were calibrated by assessing 1,440 pictures in previous studies. A defect was defined as any disruption of the integrity of the dentin (Figure 2). Only 1 defect in any of the 4 pictures obtained in each slice was sufficient to register as the dentinal defect of the root.
RESULTS
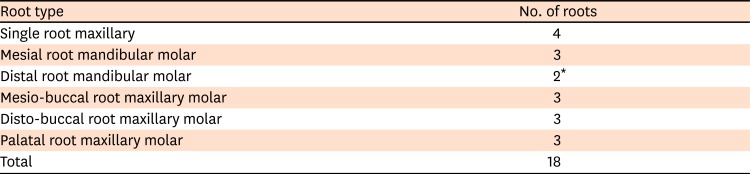
In group 1, 18 roots were obtained from patients with ages ranging from 42 to 74 years (mean 54.2 ± 7.9 years). Fourteen patients were males and 4 females. The root type for both groups is presented in Table 1.
Table 1
Distribution of root type in both groups
Group 1 had 3 defects among 18 specimens (16.7%; 95% confidence interval [CI], 0.0584–0.3923), and group 2 had 11 defects among 18 specimens (61.1%; 95% CI, 0.3862–0.7969). This difference was statistically significant (p = 0.015; Table 2).

DISCUSSION
Root sectioning methodology has been used previously in several studies to evaluate dentinal defects [4614]. This methodology destroys the root and does not allow repeating experiments in the same sample. It has been proposed that the sectioning might either create defects or propagate defects that were present in the roots before tooth removal. However, root sectioning permits the direct visualization of defects under magnification. The majority of previous studies utilizing this methodology with magnification alone showed uninstrumented specimens without dentinal defects [141516]. However, dentinal defects were more likely to be visualized in uninstrumented roots when dye was added [1718], LED transillumination was used [710], or when the root canal space was masked [9]. This study is consistent with the latter findings, and demonstrates the difficulty in making conclusions when the control groups are not carefully inspected.
Previous studies using LED transillumination methodology have shown that uninstrumented roots have dentinal defects in 47.5% and 50% of the specimens [710]. This underscores the importance of reducing extraction forces and storage time, to reach meaningful conclusions. The present study showed defects in 61.1% of the specimens when there was no control of extraction forces and storage conditions. In the periodontally compromised group (group 1), the extraction forces were presumably low and the storage in saline was brief. The percentage of specimens with defects was 16.7%, which was significantly lower than the control group. The presence of dentinal defects in these specimens may be due to the sectioning procedure or the low forces that are still needed to extract the tooth which is still problematic. Other studies using micro-computed tomography (CT) scan, a non-destructive method, also showed dentinal defects to be present in roots before root canal instrumentation [1920]. These defects or cracks that may be present in uninstrumented teeth are likely related to occlusal forces, particularly in older patients, that are difficult to quantify or control. Although these cracks or defects may propagate into a vertical root fracture without root canal treatment in some populations [21], it is rare for this to occur in western populations [22]. It has been clearly shown, however, that dentinal defects contribute to the reduction of prognosis of teeth undergoing root end surgery [2], and thus the study of their origin and characteristics is clinically important.
The possibility that extraction forces and storage time of the specimens creates the defects has been raised before [11]. It is well known that when exposed to dry conditions, dentin can become brittle, leading to spontaneous development of dentinal defects [23]. However, the effects of keeping specimens in 100% hydration for extended periods are still unclear. In this study, the specimens of group 2 were stored in saline; however, storage time of these specimens was unknown. The extraction forces applied in group 2 were also unknown. The majority of the studies did not control the time between extraction and sectioning [2425]. Çapar et al. [26] mention that the teeth have been extracted in 3 months or less, whereas another study mentioned freshly extracted without further details [16]. This issue was also emphasized in a recent review paper which stressed the fact that the majority of the studies related to creation of dentinal defects did not properly control extraction forces and storage time [12]. Despite the suggestion that storage might create dentinal defects, Adorno et al. [27] have shown that 4-week storage had no influence on creation of dentinal defect after root canal filling. In this study, the slices were obtained from sectioning done within an 1 hour interval. The imaging process was accomplished so that the specimens were kept out of saline for no longer than 1 minute to avoid dehydration. Even with a better control of storage time, group 1 still had dentinal defects in 16.7% of the specimens.
In the present study, teeth in group 1 were obtained from a Graduate Periodontology Clinic from periodontally compromised teeth presenting class II or III mobility, thus requiring minimal forces for extraction. Our findings for group 1 differ from those of previous studies [1428], which evaluated roots obtained from teeth presenting class II or III mobility [14], or extracted for periodontal reasons [28], and documented no dentinal defects. In general, previous studies have not found dentinal defects in uninstrumented roots with uncontrolled storage time and extraction force. The present study achieved a better control of these conditions expecting to have fewer specimens with dentinal defects. Masking the specimens of the present study had reduced bias of the evaluators. Arias et al. [9] also showed dentinal defects in uninstrumented roots, when the root canal space was masked. We can surmise that evaluators may not assess uninstrumented roots as carefully as they do with instrumented ones, and that this may influence the results.
Ivancik et al. [29] have demonstrated that aging is a factor that increases brittleness of human dentin. A previous ex vivo study using human teeth [30] and a recent in vivo study [31] have suggested that the age of patients is related to higher possibility of vertical root fracture. In an animal model, Rose and Svec [8] used young pigs and showed that instrumented teeth were not subjected to dentinal defects. Arias et al. [9] showed 50% of dentinal defects in a pilot study in a cadaver model; the mean age of the donors, 82 years old, has been suggested to have influenced the results of that study. In the present study, the mean age of the patients in group 1 was 54.2 years and the percentage of defects (16.7%) was lower than Arias et al.'s data [9]. Taken together, these results concur with previous studies that age of patients can play an important role in creation of dentinal defect.
CONCLUSIONS
LED transillumination assessment of freshly extracted roots with mobility class II or III showed a smaller number of dentinal defects when compared with roots with uncontrolled extraction forces and storage time. It appears that tooth extraction forces and storage conditions may contribute to the development of dentinal defects. The use of freshly extracted roots with mobility should be considered for future dental defect assessment studies.
 XML Download
XML Download