

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Dental composite resin recently became the material of choice for most patients and dental practitioners.1 However, volumetric shrinkage and fracture are still considered as major concerns with dental composites.23 In order to overcome these weaknesses, attempts have been made toward increasing both their physical and mechanical properties.4 This necessitates the comprehensive appraisal of each of its components such as the resin matrix, the filler or the filler-resin interface, and their role in affecting the material properties. Different studies have investigated this in order to improve composite properties, either by varying the particle size, percentage, or by development of the polymer matrix chemistry.45
Evolution in both filler and polymer technology in dental composite resins led to a wide selection of materials that provide the adequate properties required for each clinical situation.4 Yet, the use of dental composites in high stress bearing areas remains to be a challenge for the dental practitioner, since bulk fracture is still considered one of the primary reasons for failure.26 Bulk fill composites were introduced in an effort to improve the performance of composite resin restorations, which was inserted in 4 mm increments mainly in the posterior areas and considered to have higher physical and mechanical properties to endure the higher masticatory stresses. Moreover, the reduced treatment time decrease the risk of air entrapment or moisture contamination.7 They are also claimed to reduce cuspal deflection and promote light transmittance.78 Currently, various studies reveal the difficulty in comparing between the available materials due to variation in composition and viscosity.91011
Bulk filling composites usually have higher filler volume percentage, and sometimes a modified initiator system to ensure better curing in depth, as compared to conventional composites. While no long term clinical studies are available regarding their intraoral performance, Ilie et al. found bulk filling composites to have lower mechanical properties, except for flexural strength as compared to nanohybrid and microhybrid resin based composites.9 However, other studies found them equally successful compared to conventional composites.712 Many bulk fill composite resins have been investigated regarding different parameters like degree of conversion, polymerization stress or microleakage. Such studies have shown that bulk fill composites resins have similar properties as conventional dental composite resins.1213141516
Finan et al. studied the degree of conversion, biaxial flexural strength and Vickers hardness of two flowable bulk composites (SDR and XB), and despite the differences between the two materials, found that the properties justify their use in 4 mm increments.17 The variation in material composition and viscosity, whether flowable or non flowable bulk composites, leads to differences in physical and mechanical properties among the bulk fill composites available in the market.7 Fiber reinforcement of conventional dental composites were also introduced with the aim of enhancing their physical and mechanical properties, and increasing their resistance to fracture. The enhancement of the material properties was due to the stress transfer from the matrix to the fibers depending on the fibers length and diameter. Garoushi et al. studied their effect, and found a significant improvement in the materials physical properties.18
It was deemed important to investigate the role of fibers added to composite compared to other commonly used bulk fill composites, and to examine the extent to which fiber reinforcement would enhance the mechanical properties of the materials. Multiple laboratory investigations have been used to evaluate dental composite resins; standardized tests present the advantage of being easily reproducible in laboratories, and allowing values obtained by different institutes to be compared. Moreover, they provide preliminary information about the material suitability in the oral environment and the extent to which they conform to the indications prescribed by the manufacturer.19 Heintze et al. found that flexural strength and flexural modulus tests can be used as a good indicator for the material durability under stress, and correlate well with the clinical longevity.19 Fracture toughness test was considered by Ilie et al. as another important method that investigates the material's ability to endure stress without fracture and monitor the crack propagation inside the material before failure.11 On the other hand, Vickers hardness assay, one of the most used mechanical experiments examines the material surface hardness, and scanning electron microscope observations reveal important information about the samples used and the mode of failure of the material.9 Standard ISO flexural strength and modulus tests consider only 2 mm thickness samples. However bulk fill composites are indicated to be used clinically in 4 mm thick increments, and accordingly investigating the material at this thickness seems more appropriate.
The aim of this study was to investigate the mechanical properties of a fiber reinforced composite compared to other commonly used bulk fill composites, and to consider its performance under laboratory settings. The null hypothesis was that there is no significant difference in mechanical properties (flexural strength, flexural modulus, fracture toughness, and Vickers hardness) among the fiber reinforced composite and other bulk fill composites.
Materials and Methods
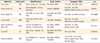
Bulk fill dental composites used in the study were X-tra base (XB, Voco GmbH, Cuxhaven, Germany), Venus bulk fill (VB, HerausKultzer, Hanau, Germany), Filtek bulk fill (FB, 3M ESPE, St. Paul, MN, USA), Surefil SDR (SDR, Dentsply, Milford, DE, USA), Tetric evoceram bulk fill (TECB, Ivoclar Vivadent AG, Schaan, Liechtenstein), SonicFill (SF, Kerr Corp., Orange, CA, USA), and a fiber reinforced bulk fill dental composite resin, EverX Posterior (EXP, GC EUROPE NV, Leuven, Belgium). The compositions of bulk fill materials used, their shade as well as their lot numbers are listed in Table 1.
For the fracture toughness test, flexural strength and modulus tests, the number of samples for each of the materials used was 6. The tested samples were polymerized using GC G-light unit (GC EUROPE NV) from both sides for 40 seconds. A modified flexural strength test was performed using bulk fill samples with 4 mm2 cross sectional areas polymerized only from the top side as done in the clinical situation. The wavelength of the light was between 380 and 520 nm with maximal intensity at 470 nm and light intensity was 1,150 mW/cm2. The specimens from each group were stored in water at 37℃ for 48 hours before testing.
Fracture toughness
To measure the fracture toughness (KIC), rectangular glass molds that were lined with polyester strips (Striproll, Kerrhawe SA, Bioggio, Switzerland) were used to prepare single-edge-notched specimens. The cured samples (3 mm × 6 mm × 25 mm) were removed without using force. A sharp central notch of specific length (a) was produced by inserting a razor blade into an accurately fabricated slot at mid-height in the mold. The slot extended down half the height to give a/W = 0.5. The crack plane was perpendicular to the specimen length. The length of the crack was checked using a stereomicroscope.

Flexural strength and flexural modulus
According to the ISO 4049, samples for a three point bending test were prepared in Teflon molds between two glass slabs, resulting in bar shaped specimens (2 mm × 2 mm × 25 mm). The test was conducted under a cross-head speed of 0.5 mm/min, with a span length of 20 mm and an indenter diameter of 2 mm. All specimens were loaded in a Universal Mechanical testing machine (Servo hydraulic - Adamel Lhomargy DY-34, MTS, Roissy-en-Brie, France). Flexural strength and modulus tests, were repeated on larger samples (n = 6, 4 mm × 4 mm × 25 mm), that were cured only from the top, using the same light and stored in water at 37℃ for 48 hours before testing.


Where Fm is the applied load (N) at the highest point of load-deflection curve, I is the span length (20 mm), b is the width of test specimens and h is the thickness of test specimens. S is the stiffness (S = F/d, N/m) and d is the deflection corresponding to load F at a point in the straight-line portion of the trace.
Vickers hardness test
The Vickers hardness test was performed with Leitz microhardness device (Leitz, Wetzlar, Germany), under a force of 200 g for 30 seconds. Ten samples for each material were prepared using a 5 mm diameter Teflon mold, with either 2 mm (n = 5) or 4 mm thickness (n = 5), placed between 2 glass plates. The materials were polymerized only on one side for 40 seconds. The excesses were removed by polishing the 2 surfaces using abrasive paper discs of decreasing coarseness from 2,400 to 4,000 grits (Struers SAS, Champigny sur Marne, France) at 3,000 rpm under water irrigation. The top surface (polymerized) and the bottom surface (non-polymerized) were marked to be identified. Each sample was tested 5 times on each side, at 24 hours after immersion in distilled water at 37℃. The Vickers hardness was calculated using the formula:
Where P (g) is the load applied, and d is the average of the 2 diagonals of the surface of the diamond indentation.
Scanning electron microscopy
Scanning Electron microscope (S800-1, Hitachi Europe Ltd., Whitebrook, Berkshire, UK) observations were conducted under ×80, ×100, and ×250 magnification to examine the fracture mode, and to measure the fiber's diameter and length. Samples were dried, sputter-coated with metal, and observed. The type of fracture was determined for each specimen.
Statistical analysis
The statistical analysis of the current data was performed using the application of one-way analysis of variance (ANOVA). The results were compared between each test and between each material type using unpaired t-test. The results are reported as mean ± SD. Statistical significance was accepted at p < 0.05.
Results
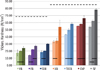
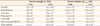
Fracture toughness and Vickers hardness of tested composite materials are presented in Figures 1 and 2. Flexural strength and flexural modulus are presented in Table 2. The fiber reinforced composite EXP had significantly higher fracture toughness value (3.1 MPa·m1/2), compared to other bulk composites except for FB (2.52 MPa·m1/2) and VB (2.26 MPa·m1/2) where no significant difference was found with EXP. In the normalized flexural strength test (2 mm × 2 mm × 25 mm), SF (157.6 MPa), EXP (153.6 MPa), XB (150.4 MPa) and FB (140.0 MPa) were not statistically different, and these have significantly higher flexural strength values compared to other tested composite materials, except for FB which was similar to SDR. EXP had significantly higher flexural modulus (14.6 GPa), while SF (12.47 GPa), TECB (10.87 GPa), and XB (10.65 GPa) were not significantly different and came in second position. On the other hand, VB (5.02 GPa) had the lowest statistically significant value.
Considering the modified test (4 mm × 4 mm × 25 mm), there was no significant difference from those obtained in the original test, except for XB and they had the same order of the strength values from SF (147.67 MPa), EXP (140.04 MPa), and FB (139.62 MPa). On the other hand, the flexural modulus values decreased significantly in comparison with the normalized test, attaining almost half the original value, while remaining in the same order, with the highest flexural modulus for EXP (6.89 GPa), together with SF (6.55 GPa), followed by XB (5.7 GPa) and FB (4.01 GPa), which were less affected in comparison with original test.
Vickers hardness values revealed that SF had the highest value followed by EXP. The decrease in hardness between the surface and 2 mm and 4 mm depths were not significant for EXP, TECB, and VB, while other bulk composites revealed a significant difference between the curing depths.
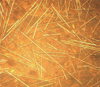
SEM analysis revealed that the fibers stop the crack propagation along the fracture line, as shown in Figure 3.
Discussion
According to the results obtained in the current study, the null hypothesis was rejected, that is, fiber insertion into composite leads to significant increase in physical and mechanical properties, such as flexural strength, flexural modulus, fracture toughness, and Vickers hardness.
In this study, flexural strength and modulus were investigated. These tests are considered to be good indicators of the material resistance to fracture in normal masticatory conditions, taking in account the great variability in the results obtained between studies.1920 The results obtained are in accordance with previous studies conducted on bulk composites. SF, EXP, XB, and FB had significantly higher flexural strength values, compared to VB and TECB which had the lowest.91821 Moreover, as shown in previous works, the filler volume percentage is closely related to the flexural strength and flexural modulus values.91821 This can be shown for SF with the highest filler volume percentage (83%) ranking the highest, TECB (61%) and XB (58%) follow next, while VB with the lesser filler volume percentage (38%) ranking the lowest. Interestingly, EXP (53.6%) performed relatively better in these two tests compared to its filler volume percentage, showing the role of the fibers in increasing the material stiffness and resistance to bending force during testing and probably during function.
In this work, the modified flexural strength and modulus tests were done on 4 mm increments cured only from the top side in an effort to mimic the clinical situation. This would eventually mean less matrix polymerization and, accordingly, a larger role of the filler type and percentage in the material behavior. The results obtained show that the flexural strength values remained significantly unchanged. In comparison to the original test, significant decrease in the flexural modulus values of the composites tested indicated a marked decrease in rigidity. This is probably due to an increase in thickness of the increments and decrease in the overall matrix polymerization. A probable explanation would be that, as a result of less matrix polymerization and the consequent lack of rigidity, the modified test samples were able to withstand flexure even at greater load relative to greater sample thickness (hence unchanged flexural strength) but with more deformation before final failure (hence lower modulus of flexure). These results, when confirmed with further studies, would throw more insight on an important aspect regarding the amount of deformation and the distortion of the material due to the decreased stiffness, most notably at the interface region. This would also provide some explanation for the discrepancies found between results obtained in the laboratories and those from clinical studies in which bulk materials are inserted in larger and thicker increments and cured only from one side.19
Results obtained acknowledge the role of fibers in increasing the material's resistance to fracture, and coincide with those of previous studies.1822 The single edge notched beam method used in this study is one of the most commonly used fracture toughness test methods, which are used to predict resistance to fracture. The method is widely used in dental material research and is usually conducted by means of a 3 point bending apparatus, and the sharp crack created could be easily measured. This method is also very sensitive to the notch width and depth, thus making comparison difficult between different studies.1118 In the present work, no correlation was found between the fracture toughness value and the filler volume percentage or the filler particle size.
The enhancement of the material properties was explained to be due to the stress transfer from the matrix to the fibers and also due to the action of the fibers in stopping crack propagation through the material.23 It was found that the mere insertion of fibers is not enough to enhance the composite properties, that is, the fibers length and diameter play a critical role in this mechanism. Peterson found that fibers incorporated into a material, greatly enhances its mechanical properties, on the condition that the fibers have a length that exceeds a certain minimum length. This is known as the critical fiber length, which could be calculated using the following formula:24

Where the critical length (lc) equals the ultimate tensile strength of the fiber (f) multiplied by the fiber diameter (d), and divided by twice the shear strength of the matrix interface (c)
The physical explanation of the strengthening and stiffening mechanism is that since the matrix has a much lower modulus than the fiber, the matrix strains more. The critical fiber length is therefore the minimum length at which the center of the fiber reaches its ultimate tensile strength when the matrix reaches its maximum shear strength. Accordingly, composite with fibers below critical length fail to show enhanced properties.18 In the present study, we were able to measure the fiber length and diameter using stereomicroscopy and SEM, and we found that EXP had a fiber diameter of 16 µm and a wide range of fiber length, with the average length lying between 1 and 2 mm similar to the values found in previous studies, thus exceeding the fiber length required.18 The fiber length and orientation can be shown in Figure 4.
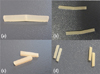
One interesting observation found from the fracture toughness and the flexural strength test samples alike was that all fiber reinforced composite EXP samples remained attached, even after failure of the sample and formation of crack line, unlike the samples from other bulk fill brands which separated in two pieces the time the failure load was reached, as can be seen in Figure 5. Scanning electron microscope observations performed on fractured samples show the fibers traversing the crack line and between the fractured parts, as can be seen in Figure 3. Further investigation of this property is important clinically, since not only it shows the material resistance to fracture, but also its resistance to displacement at the more vulnerable interface, thus preventing cavitation and food impaction. Moreover, this property would render the material with better potential for repair.
The Vickers microhardness test samples show that SF, EXP, TECB, and XB have the highest values compared to SDR, FB, and VB. It is worth noting that though this method was criticized as an unreliable indicator of the curing quality, and that it overestimates the depth of cure. Flury et al. have shown that Vickers microhardness could be considered as an accurate tool for estimating the polymerization depth for bulk composite resins.2526 Moreover, only SF and EXP had bottom surface hardness values that exceeded the 50 VHN considered ideal.27 However, EXP is the only composite with Vickers hardness value at 4 mm depth that exceeded the 80% ratio compared to the top surface hardness as required in literature.26272829 The results thus obtained provide evidence that EXP could be used in 4 mm increments for tooth cavity fillings.
The present results were obtained in optimized laboratory settings, however, clinical conditions are not similar and the aspects like insertion and handling could have a potential effect on the mechanical properties of the materials and their performance in vivo. Another important factor that should be taken into consideration as one of the limitations of the current study is the fiber alignment inside the composite in relation to the acting force, which is not necessarily consistent with the laboratory simulations performed during in vitro testing. Some of the important aspects considering the materials polymerization contraction and contraction stress were not included in the study. Further investigations should be conducted to test other material properties. According to the results obtained in this work, the fiber reinforced composite tested may be used as a restorative material in stress bearing areas. In order to acknowledge the results obtained with the present study, this should be followed by long term clinical studies to assure the materials performance under normal clinical conditions.


 XML Download
XML Download