

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
An intracranial or Spinal Subarachnoid Hemorrhage (Sah) Can Result From The Rupture Of An Aneurysm In The Anterior, Posterior, Radicular, Or Radiculomedullary Cervical Spinal Arteries. Hemodynamic Stress Caused By Arteriovenous Malformation And Coarctation Of The Aorta Are Well-known Etiologic Factors In Formation And Rupture Of A Spinal Artery Aneurysm.3)4)6)7)12)16) However, Occurrence Of An Sah Due To The Rupture Of An Isolated Aneurysm In The Cervical Anterior Spinal Artery Is Very Rare. We Report On A Case Of An Sah That Resulted From The Rupture Of An Aneurysm In The Branch Of The Anterior Spinal Artery In A Patient With End-stage Common Bile Duct Cancer. We Also Performed A Literature Review of relevant cases.
CASE REPORT
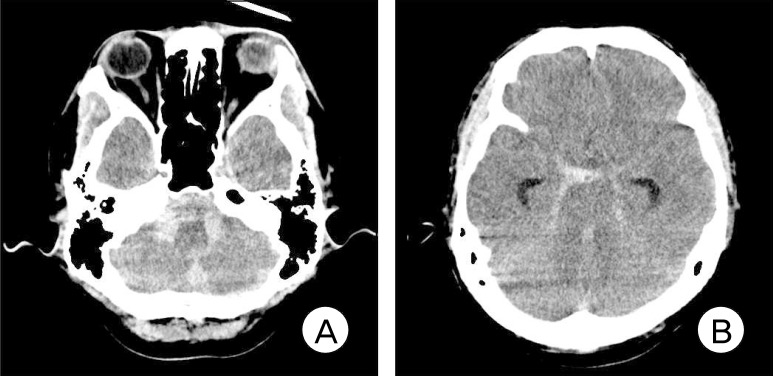
A 47-year-old male was transferred to our emergency room in a semicomatose state. Initially, he presented with posterior neck pain that gradually became more aggravated during the transfer. Brain computerized tomography scans showed subarachnoid and intraventricular hemorrhages that were denser in the cisterns around the pons and medulla than in the basal and anterior interhemispheric cisterns (Fig. 1). By the next morning, the patient's condition had improved from a semicomatose to a drowsy state. His family requested further treatment at this time.
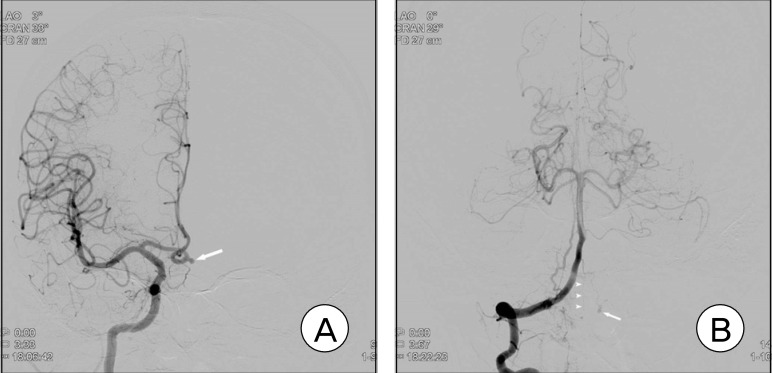
We performed an immediate cerebral angiography. We found an aneurysm in the anterior communicating artery and performed embolization of the aneurysm using detachable coils (Fig. 2A). We did not notice a small aneurysm in the branch of the anterior spinal artery until the following day during a review of the angiograms (Fig. 2B). We expected spontaneous occlusion of the aneurysm; therefore, we decided to follow this aneurysm with cerebral angiography. We took this course of action because the family did not want the aneurysm to be clipped. In addition, we believed that endovascular treatment carried the risks of both parent artery occlusion and additional hemorrhaging.
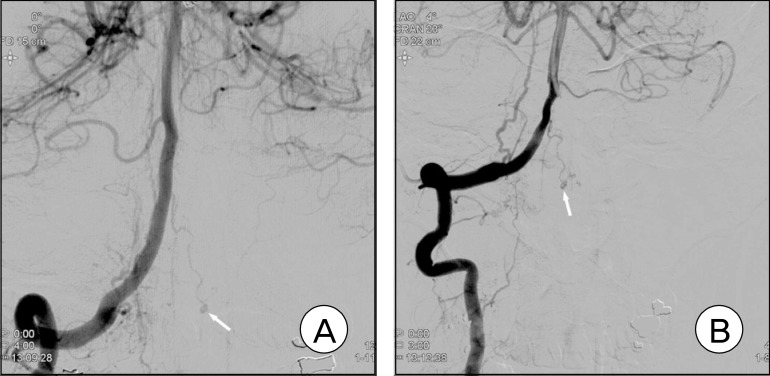
On the sixth day of hospitalization, follow-up cerebral angiography showed that the aneurysm was still present in the anterior spinal artery branch with a small filling defect in the aneurysm sac (Fig. 3A). Therefore, we decided to continue to follow the aneurysm with cerebral angiography. Due to progression of the patient's end-stage common bile duct cancer, his condition slowly worsened. We performed a final cerebral angiography on the 23rd day of hospitalization. The angiograms showed no significant interval change in the aneurysm from previous examinations (Fig. 3B). The general condition of the patient continued to deteriorate. He returned to his hometown where he died of the cancer on the 103rd day after the SAH. No rebleeding from the aneurysm was observed.
DISCUSSION
Both arteriovenous malformations of the spinal arteries and coarctation of the aorta are known to cause hemodynamic stress on the arteries and formation and rupture of aneurysms.3)4)6)7)12)16) However, rupture of an isolated aneurysm in the anterior spinal artery has rarely been reported. To the best of our knowledge, only eight cases of SAHs resulting from the rupture of an isolated aneurysm in the cervical anterior spinal artery have been reported.8)9)14)15)17)18-20) In our case, the aneurysm was located in the branch of the cervical anterior spinal artery in a patient with common bile duct cancer. To the best of our knowledge, this is the first case in which an SAH resulted from the rupture of an aneurysm that was located in the branch of the anterior spinal artery in a patient with common bile duct cancer.
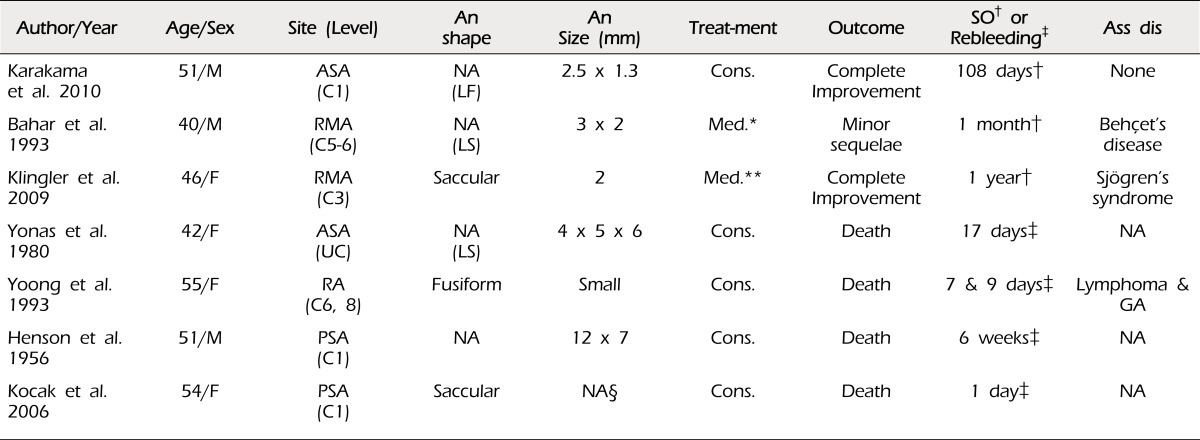
The strategy for treatment of spinal artery aneurysms remains controversial. Among the eight reported cases of ruptured anterior spinal artery aneurysms, two cases were treated conservatively,8)20) and one of these two cases resulted in death.8) A review of the literature identified three cases of aneurysms located in the cervical radicular,5)11)21) radiculomedullary, or posterior spinal artery, which resulted in death among five conservatively treated cases.1)5)10)11)21) In contrast, all patients who were treated with embolization, surgical resection, or aneurysm clipping recovered completely or with some sequelae. Thus, we agree with the opinion that surgical or endovascular intervention is the ideal treatment of choice for a ruptured cervical anterior spinal artery aneurysm.8)
However, conservative medical treatment has been successful in some cases. In the case of a patient with a small, ruptured aneurysm measuring approximately 2.5 × 1.3 mm in size and located in the anterior spinal artery at the first cervical vertebra level, the aneurysm disappeared from the angiograms after 108 days of conservative management. The authors chose conservative treatment because they thought that obliteration of the aneurysm would be difficult without disrupting the blood flow of the parent artery. Due to its spontaneous disappearance, the authors assumed that the aneurysm was a dissecting aneurysm.8) In a second case, a ruptured aneurysm measuring approximately 3 × 2 mm in size and located at the C5-6 radiculomedullary artery was found in a patient with Behçet's disease; a follow-up angiography one month later showed no aneurysm following high-dose methyl-prednisolone therapy, which was initiated on the day of admission.1) Another case report described a ruptured aneurysm in a patient with Sjögren's syndrome. The small saccular aneurysm, which was located in a radiculomedullary branch of the right vertebral artery at the C3 level, had a diameter of approximately 2 mm. The authors presumed that the aneurysm had formed due to the immunological vasculitis that is associated with Sjögren's syndrome and treated the patient with glucocorticoids, cyclophosphamide and azathioprine. The aneurysm was not detected during digital subtraction angiography one year after the SAH.10) In addition, Longatti et al. considered the mass effect of aneurysms or blood clots as the only indication for surgical treatment.13)
Therefore, conservative medical treatment can be another management strategy when the aneurysm is associated with dissection or immunological vasculitis, as in Behçet's disease and Sjögren's syndrome. This may be particularly true if the parent artery cannot be preserved, the patient's condition is not suitable for surgical treatment, or endovascular treatment poses more hazards than benefits. Spontaneous disappearance of an aneurysm between one month and one year after the SAH has been reported. Thus, waiting at least one year for spontaneous occlusion of the aneurysm to occur is possible.1)2) We could not confirm the disappearance of the anterior spinal artery aneurysm, however, the aneurysm did not re-rupture during the 103 days after the SAH. In addition, the caliber of the parent artery of the aneurysm can be considered too small to make a true saccular aneurysm. Thus, the author believes that the aneurysm in this case may have been a dissecting aneurysm.
An aneurysm rupture at the cervical spinal level results in development of intracranial hemorrhages as well as spinal SAHs. Recurrent hemorrhage has been the cause of death in all patients who have received conservative treatment, and rebleeding occurred from the day of admission to the 17th hospital day.11)21) Thus, an operative intervention should be performed immediately, if indicated, as in cases of intracranial aneurysm rupture.
CONCLUSION
An patient with end-stage cancer with an SAH due to the rupture of an aneurysm in the branch of the anterior spinal artery received conservative management. This expectative strategy was chosen because his family did not want open surgical management and endovascular treatment might carry the risk of parent artery occlusion and injury. The patient survived for 103 days after the SAH without a re-rupture of the aneurysm. A conservative management strategy is a viable option for patients with conditions that are unsuitable for surgical or endovascular management.
 XML Download
XML Download