

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Turner syndrome (TS) is diagnosed in females with partial or complete absence of one X chromosome (45,X karyotype). TS is a symptom complex, which also called X0 syndrome or Bonnevie-Ullrich syndrome, and was first described in 1938 by Ullrich and Turner.1 This syndrome occurs in one out of every 2000 to 3000 live female births.2 TS is characterized by numerous medical and craniofacial challenges.3 Patients with TS are at risk of congenital heart defects, developing hypertension, thyroid disease, diabetes mellitus, osteoporosis, congenital lymphedema, renal malformation, sensorineural hearing loss, obesity, and atherogenic lipid profile.4 Patients usually have normal intelligence; however, they may have problems with social and psychomotor skills.4,5 Clinical signs for TS include shortness, gonadal dysgenesis, congenital lymphedema, prominent thorax or broad chest, short neck, hypoplastic nails, low posterior hairline, epicanthal fold, ptosis of the eyelids, and prominent and low-set ears. The phenotypic characteristics of children and adolescents that lead to medical consultation include short stature, failure to initiate puberty, and absence of breast development.6,7 The absence of the X chromosome in girls with TS affects the shape and the size of craniofacial structures. The most frequent oral and craniofacial findings of TS patients are hypoplastic mandible and high palatal vault.8 A reduced size and an altered morphology of both the dental crown and root in primary and permanent teeth have been reported as well.6,9
Prolactinomas (prolactin cell adenoma) are the most frequently diagnosed functioning pituitary tumor. They represent approximately 30% of all pituitary tumors. Prolactinomas are the only pituitary tumors in which a reliably effective medical therapy is available.10 Prolactinomas are generally classified according to size as microadenomas (less than 10 mm in diameter) or macroadenomas (more than 10 mm in diameter). Primary (in children) or secondary amenorrhoea due to hyperprolactinaemia and neurological symptoms including headaches and visual impairment are the main clinical features of prolactinoma.11
Eagle syndrome (ES) is characterized by a elongated styloid process. The syndrome can occur unilaterally or bilaterally when the styloid process or the ossified stylohyoid ligament is longer than 30 mm.12,13 Symptoms of ES include foreign body sensation, dysphagia, change in voice, sensation of hypersalivation, throat, neck, and jaw pain secondary to an elongated styloid process, and/or calcified stylohyoid ligament.13-15
In the present article, a unique case of TS accompanying elongated styloid process specific to ES and prolactinoma was illustrated with cone-beam computed tomographic (CBCT) examination.
Case Report
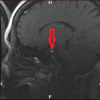
A 40-year-old female patient was referred to ukurova University Faculty of Dentistry with the requisition of orthodontic treatment and odontalgia due to dental caries. Medical anamnesis of the patient revealed that she had TS accompanying prolactinoma and osteoporosis (Fig. 1). The patient was also receiving care from the endocrinology, neurology, and physical and rehabilitation medicine departments at the university hospital. A general physical examination showed that the patient height was 140 cm and weight 40 kg with normal gait and vital signs. According to the patient's medical history, it was revealed that she had undergone ear surgery due to otorrhea and recurrent otitis media at the age of 6. She had been diagnosed with TS at the age of 12 by endocrinologists due to the patient's complaints of amenorrhea and shortness in stature. At the age of 16, prolactinoma had been diagnosed with the complaints of visual disturbances and chronic headaches. The patient had been on medical treatment (dopamine agonist therapy) for a period of about 8 years for the tumor. She had responded to the medical treatment well without needing any surgical treatment. However, the last cranial magnetic resonance imaging (MRI) of the patient showed a recurrence of the prolactinoma. She has been continuing to follow up at the neurology clinic and receiving medical treatment with a dopamine agonist for her microadenoma (Fig. 2).
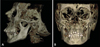
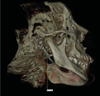
The patient's general clinical symptoms were hirsutism, amenorrhea, congenital speech difficulties, partial hearing loss, sinusitis, headache, neck and throat pain, and dysphagia (Fig. 3). She used calcium supplements, oral bisphosphonate, and vitamin D for osteoporosis; ethinyl estradiol for increasing growth velocity; cyproterone for hirsutism; and lansoprazol for peptic ulcer.
The intraoral examination and panoramic radiograph demonstrated that the patient had malocclusion, maxillary micrognatia, high and narrow palatal arch, retrusive mandible, bifid uvula, prevalent microdontia, hypoplastic first maxillary premolars, and short dental roots (Figs. 4 and 5). The dental caries of the patient were restorated in the pediatric dentistry clinic.
We utilized the patient's CBCT (Iluma cone-beam CT Scanner, Imtec Imaging L.L.C., Ardmore, OK, USA) scan, which was performed for orthodontic evaluation, and detected a number of craniofacial abnormalities specific to TS. The dental tomographic examination showed the crowding of teeth, especially in the maxillary anterior region, because of the maxillary narrowness. The maxilla and mandible were both micrognathic. Relative mandibular retrusion, malocclusion and open-bite were observed (Fig. 6). An elongated styloid process (length of 32.7 mm) was also detected on the right side (Fig. 7).
The patient was referred to the otolaryngology department of the university hospital for a detailed examination and assessment of speech problems. The temporal bone axial and coronal computed tomography (CT) reports noted that the tympanic membranes looked thick and retracted bilaterally; on the left side, peripheral soft tissue density appeared at the external auditory canal. Otoscopic examination showed that the right tympanic membrane was intact and calcified plaques were visible around the tympanic membrane. The left tympanic membrane was perforated, and there was an adhesion to the head of the stapes. According to endoscopic rhinoscopy, the nasal septum deviated to the left side; there was also a slight polypoid degeneration in the middle nasal conchas and adenoid vegetation at the nasopharynx. Otolaryngologists recommended surgical treatment for ES, but the patient rejected the surgical intervention.
Discussion
There is evidence in the literature that genetic factors could contribute to dental and craniofacial abnormalities.8,16,17 Patients with TS have a high palatal arch and cleft palate, sharpened canines and premolars, atypical cusps, root length alterations, and hypoplastic crown of premolars.6,8,17 "Turner's teeth" are described as permanent teeth, especially in the case of second mandibular premolars, that show hypoplasia in their crowns.18 Our patient had hypoplastic maxillary first premolars, which could be described as Turner's teeth. Some other specific abnormalities of TS, including imbalanced craniofacial skeletal growth with flattening of the basal skull, reduction of the transversal dimension of the maxilla, and retrusion of both jaws, has also been described.16 A high arched palate, a higher frequency of cleft palate occurrence, and malocclusion have been described.8,17 Orthodontic anomalies of patients with TS were also reported by Harju et al.19 They found that the occlusion of these patients seemed to be more abnormal than that of women without TS. It might be speculated that enamel genes on the X chromosome are involved in occlusal development.19,20 According to a hypothesis of Gorlin et al, the absence of an X chromosome also has an effect on mandibular growth relative to maxillary development.21 Intraoral examination and CBCT investigation of our patient showed a number of craniofacial abnormalities specific to TS and an unexpected elongated styloid process specific to ES. It was thought that some of the patient's complaints, including headache, throat and neck pain, and dysphagia, might have been based on ES. To the best of our knowledge, there has been no such case of Turner syndrome accompanying ES and prolactinoma reported in the literature.
In conclusion, patients with TS carry various risks that make treatment more complicated; thus advanced imaging techniques for proper treatment and follow-up would be extremely important. In the light of CBCT examination, craniofacial abnormalities specific to TS and accompanying syndromes could be illustrated in detail.




 XML Download
XML Download