

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
In clinical orthodontics, the size, position, and relationships of craniofacial structures are evaluated using lateral cephalometric radiograph as an essential tool in order to understand the etiology of malocclusion, which provides data to make a plan for the correction of the problems.
Since cephalometric radiographs were introduced in clinical orthodontics in 1931, they have been used as an essential tool to study on the craniofacial growth, to make orthodontic diagnosis and treatment plan, to evaluate treatment results, and to predict craniofacial growth. However, the two-dimensional (2D) images had a limitation as diagnostic tool in complicated dentofacial deformities. Therefore, additional images such as postero-anterior cephalometric radiograph and submentovertex radiograph were used as well. Nevertheless, in such complicated dentofacial deformity cases, the combination of 2D images could not provide sufficient information. However, three-dimensional (3D) reconstructed images using CT have been recently introduced, which made it possible to evaluate 3D relationship of anatomic structures properly and to make a decision of 3D surgical plan. In addition, 3D image data can be used for surgical simulation using 3D reconstructed images on computer monitor, real surgical simulation onto the stereolithographic model produced with 3D image data, and construction of surgical wafer or guide. In the future, such technology would provide more realistic surgical simulation on computer monitor, easy evaluation of possibility of limitation for such simulation, and decision of final surgical plan and construction of surgical wafer in a single serial process.
Conventional multi-detector CT (MDCT) has been used to obtain image data from different angles of the body, however it has limitations such as cost, high radiation, and difficulty to access. Therefore, it may have limited uses for patients with severe dentofacial deformities requiring surgical approach. However, the recently developed cone-beam CT (CBCT)1-3 for dental use has increased practical use in clinical orthodontic field because it has advantages such as cost-effectiveness, less radiation dose, and more accessibility compared with MDCT. It was reported that CBCT was useful in the general orthodontic field such as orthodontic diagnosis through orthodontic simulation4 and 3D evaluation of upper respiratory system.5 Moreover, CBCT can be used as a useful tool to provide superimposition for evaluation of growth, treatment and stability, or information about impacted teeth or bone quality needed for effective orthodontic treatment.6,7 So far, many diagnostic me-thods using 3D landmarks and reference planes on 3D sur-face rendering images have been introduced.8-15 The storage of information and data of the dentofacial structure of normal or average population might help the diagnosis of orthodontic patients using 3D cephalometry directly in the future. For this purpose, the reproducibility and accuracy of the landmark identification on 3D CT surface rendering image should be confirmed. Therefore, this study was performed to evaluate the accuracy of linear measurements on the 3D images acquired from MDCT and CBCT.
Materials and Methods
Twenty-four dry skulls were used in this study. In the skulls which lost the upper or lower incisors, acrylic artificial teeth mixed with barium powder were positioned into the alveolar socket in order to mimic the incisors (Fig. 1). Rubber impression material was placed between the condylar head and the articular surface in order to separate them, and the mandible was fixed to the cranium and maxilla using a rubber band. Subsequently, MDCT and CBCT were taken with appropriate position according to the image acquisition protocol. Image taking protocol for MDCT with Somatom Sensation (Siemens, Erlangen, Germany) was set at 120 kVp, 50 mA, 2.8 seconds scan time, 512×512 matrix, 0.75 mm slice thickness, 0.5 mm reconstruction interval, and 256 mm length. That of CBCT with 3D eXam Dental CT (Kavo, Biberach, Germany) was 23×17 cm FOV size, 8.5 seconds scan time, isotropic voxel of 0.3 mm axial slice thickness (Fig. 2). These axial data were stored as DICOM file.
Using 14 landmarks (Table 1), the direct (physical) measurements on the dry skulls were compared with the image-based measurements on the 3D surface rendering images acquired from the MDCT and CBCT, that a total of twenty -one distance measurements were performed: nine distance measurements on the mid-sagittal surface (S-Na, Ba-Na, Ba-ANS, ANS-PNS, Na-ANS, Na-A, Na-B, Na-Pog, Na-Me) and six distance measurements between the bilateral landmarks (Pog-Go, Pog-Co, Go-Me, Go-Co, Go-Gn, Po-Or). Since Sella (S) is not a point landmark with bony base, it could not be defined in both of the direct and image-based measurement. In this study, S was replaced by the midpoint of the floor of sella turcica. Although Condylion (Co) has variable definitions according to the projection, it was defined as the most superior point of the mandibular condyle in the sagittal and frontal view in this study. The direct measurements were performed using a customized digital caliper (Fig. 3) and the image-based measurements using OnDemand™ (ver. 1.0, Cybermed, Seoul, Korea) software on 3D surface rendering images of the MDCT and CBCT (Fig. 4).
In identifying the landmarks on 3D CT surface rendering image, the adjustment of threshold of image was helpful to detect the bony structures. In this study, all of the landmarks except S on the MDCT images could be identified at 0 HU threshold value, and the bony continuity of sella turcica could be identified at -500 HU. Since every dry skull had different thickness on sella turcica, the threshold of each image had to be adjusted. For the CBCT images, all of the landmarks except Or and S could be identified at 0 HU threshold value, while Or could be seen as continuous surface at -250 HU, and S at -500 HU.
The anterior mid-sagittal landmarks such as Na, ANS, A-point, B-point, Pog, and Me were identified considering both of the frontal and lateral view of 3D surface rendering image. Other inner landmarks such as PNS and Ba were defined by rotating the 3D image so that the bony edge could be readily identified. Also, all the mandibular landmarks were identified using the segmentation image removing the cranial and maxillary parts of the 3D images. All the measurements were taken by one orthodontist three times at four-week interval to exclude learning effect. The direct measurements on the dry skull were compared with the image-based measurements on 3D surface rendering image.
With above data, the repeated measurements were assessed respectively to evaluate their reproducibility, and comparison was performed between direct measurements and image-based measurements with MDCT and CBCT to investigate their accuracy. The reproducibility of the measurements was analyzed using repeated measures ANOVA and Intra-class correlation coefficient (ICC) and the measurements were compared by Student t-test. All statistical analyses were performed using SPSS for Windows (ver 10.0, SPSS Inc., Chicago, USA).
Results
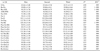
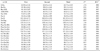
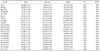
The repeated values of the direct and image-based measurements on the 3D CT images with MDCT and CBCT indicated excellent reliability with a high ICC, that the lowest values were 0.984, 0.990, and 0.0965, respectively (Tables 2-4). In the repeated measures ANOVA, there were statistical difference in five measurements (S-Na, Ba-ANS, Pog-GoRt, Pog-CoRt, Go-GnRt) of the direct measurement (Table 2), in six measurements (Ba-Na, ANS-PNS, Pog-GoRt, Pog-GoLt, Co-GoRt, Go-GnRt) of the image-based measurement on MDCT 3D reconstruction images (Table 3), and in one measurement (ANS-PNS) of that on CBCT 3D reconstruction images (Table 4). However, the differences of mean value were small; under 0.3 mm, 0.6 mm, and 0.2 mm, respectively.
Also, there was no statistical difference between the direct measurements on dry skull and the image based measurements on both types of 3D CT surface rendering images (P>.05) (Table 5).
Discussion
CT can be used not only for partial information for regional pathology5-7 but also for general information that makes it possible to make diagnosis and treatment planning, to perform surgical simulation,16,17 and to make stereolithographic model of dentofacial deformity. As CT technology has been progressed, it has been used in general orthodontic field such as orthodontic diagnosis through orthodontic simulation4 as well as surgical procedure for dentofacial deformity. Therefore, 3D CT surface rendering image has to guarantee the accuracy as a virtual image of real craniofacial structure.
The three dimensional accuracy of cephalometric landmarks on 3D surface rendering image has been studied using MDCT13,18-30 and CBCT.31-33 There were some categories in those studies; (1) identification of cephalometric landmarks on 3D surface rendering images and evaluation of the reproducibilites,19,25,28,29 and (2) identification of landmarks and comparison of those measurements on both dry skull and 3D surface rendering images.18,20-24,26,27,30-33
In the future, landmark identification and measurement on 3D CT surface rendering images may be the most important procedure in orthodontic diagnosis and treatment planning. Therefore, this study aimed to investigate the accuracy, reproducibility, and possibility of errors in those procedures. Also, this study compared the differences of the results between MDCT and CBCT. For this purpose, the landmarks in this study were selected in commonly used landmarks for both 2D images and 3D images, with agreement of definition.
As computer and CT-related technology have been progressed, it has been reported that the error of measurement originated from the image acquisition, processing, reconstruction, and display procedure has decreased and that the error of repeated measurements was generally less than 2 mm.13,18-33 However, it was reported that landmark identification on 3D surface rendering images would be quite different from that on 2D images.31,34
In this study, a total of twenty-one measurements were performed to examine the reproducibility of the repeated measurements and to compare the image-based measurements with the direct measurements on dry skull as gold standard: nine distance measurements on the midsagittal surface (S-Na, Ba-Na, Ba-ANS, ANS-PNS, Na-ANS, Na-A, Na-B, Na-Pog, Na-Me) and six distance measurements between the bilateral landmarks (Pog-Go, Pog-Co, Go-Me, Go-Co, Go-Gn, Po-Or). As shown in Tables 2-4, all the assessments under the direct measurement and image-based measurement of 3D CT surface rendering images with MDCT and CBCT revealed good reproducibility (high ICC). As shown in Table 5, all twenty-one measurements showed no differences between the measurements on dry skull and both types of 3D surface rendering images (P>.05).
The poor reproducibility of 3D landmarks identification might be originated from the contributing factors such as the characteristics of specific landmarks, errors related with CT images, and errors related with image acquisition protocol. Regarding the factors related with reproducibility of landmarks, Olszewski et al35 classified the landmarks into four groups, from group 1 (very high reproducibility) to group 4 (low reproducibility) according to their interobserver reproducibility originated from the characteristics of the landmars. According to their report, the landmarks in this study could be classified as follows. ANS was group 1, A point, Ba, S, Me, and Na were group 2, Go, Or, Po, and B were group 3, and Pog was group 4. Also, Williams and Richtsmeier26 classified the mandibular landmarks into "fuzzy", "constructed", and "biologic" according to their characteristics, that "fuzzy" and "constructed" landmarks revealed less reliability than "biological" landmarks. In this study, Gn, Pog, and Co belonged to "fuzzy" landmarks, Go belonged to "constructed", and there was no "biological" landmark. Since Na indicated the intersection of the internasal and the frontonasal suture on 2D cephalometric lateral image, vertical error might primarily occur in identifying the landmark on plain radiograph,20,31,36 while on 3D image, it might be difficult to establish the suture location on the mid-sagittal plane due to the loss of detail on the rendering image. Also, Go also revealed low reproducibility in the y-directions, and Or and Co in the x-direction on 3D images.37
The second contributing factor related to the errors was the characteristic of CT images.25,32,38 Partial volume effect19 of CT image could affect the error in identifying sharp and small landmarks such as ANS or PNS. This phenomenon appeared strongly when using dry skull, which 3D measurements were always less than the direct measurements.38 In our study, the slice thickness of MDCT was 0.75 mm, therefore the relatively thin slice might reduce those errors of the measurements.8,24,27,30,39
The third contributing factor related to the errors was the type of image acquisition. CBCT produces 3D CT images based on data acquired from a single rotation of cone-shaped X-ray tube and detector around subject.1-3 These complete series from a single 360° rotation scan is referred to as the projection data, and the number of images comprising the projection data is determined by the frame rate, the completeness of the trajectory arc, and the speed of the rotation. More projection data might provide more information in reconstructing the image. However, there was a study that showed no difference in accuracy even the number of image projections was reduced to 153.33 In this study, the image acquisition protocols were set at the commonly used protocol of patients. These protocols might result in no significant differences between direct and image-based measurements on 3D images. However, it should be considered that the accuracy of measurement might be decreased by the degradation of image quality due to soft-tissue attenuation, metallic artifacts, and patient motion. In addition, patient posture during image acquisition and head-fixing device might result the errors.32
It was reported that the landmark identification on 3D surface rendering images was more realistic and accurate than that on 2D images because the stereoscopic images could be displayed and rotated in intended direction for landmark identification. Some landmarks might be difficult to localize when using only CT axial slices.19,40 The accuracy of 3D CT was reported as higher than that of 2D CT images.21,41,42 However, some landmarks such as Me and Zy were reported to be more accurate when identifying on 3D surface rendering images in conjunction with 2D images.27 A new 3D cephalometric method, direct identification of landmarks on 3D surface rendering images,13 was regarded as an important intermediation to link 2D cephalometric radiographs and 3D images.
Available 3D images without any distortion have advantages to overcome the limitation of 2D images. Since 3D cephalometric method would be commonly used soon, the appropriate landmarks for 3D analysis should be developed. Also, their reproducibility and accuracy should be evaluated, and consensus on the landmarks should be made. In conclusion, this study evaluated the reproducibility and accuracy of identification of common cephalometric landmarks on 3D surface rendering images, and 3D surface rendering images using MDCT and CBCT were appropriate for 3D measurements.






 XML Download
XML Download