

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ellis-van Creveld (EVC) syndrome is a rare congenital genetic disorder having autosomal recessive inheritance. Credit goes to Richard W.B. Ellis and Simon van Creveld for describing the syndrome in detail in 1940, and they called it as chondroectodermal dysplasia. It is a syndrome affecting the Amish population of Pennsylvania in USA with the prevalence rate of 1/5,000 live birth. In non-Amish population, the birth prevalence is 7/1,000,000.1 It is caused by mutation in the EVC gene as well as by a mutation in a nonhomologous gene, EVC2, located close to EVC gene in a head-to-head configuration.2 The syndrome is characterized by bilateral postaxial polydactyly of the hands, chondrodysplasia of long bones resulting in acromesomelic dwarfism, ectodermal dysplasia affecting nails as well as teeth and congenital heart malformation.3,4 This report demonstrates a typical EVC syndrome in a 12-year-old Indian girl.
Case Report
A 12-year-old female patient visited the Department of Oral Medicine and Radiology, Yenepoya Dental College, with a complaint of missing anterior teeth since three years ago. She had a history of exfoliation of decidious teeth due to mobility three years ago and there was no eruption of the permanent teeth. There was a history of presence of two mandibular natal teeth which were exfoliated two weeks after birth. Her parents had no consanguineous marriage, however her elder sibling died of similar medical problem. Her medical history revealed that she had visited genetic clinic and they have diagnosed her with Ellis-van Creveld syndrome. She also had dyspnoea because of congenital lobar emphysema for which she had undergone left upper lobectomy when she was one and half year old.
Her general physical examination showed bilateral postaxial polydactyly of hands (Fig. 1A). She could not make a tight fist. She had hypoplastic finger and toe nails (Figs. 1B and C). There was wide gap between the big toe and other toes (Fig. 1C). Intraoral examination showed V-shaped notching of the upper lip at the mid line (Fig. 2A), absence of mucobuccal fold in maxillary and mandibular anterior region (Figs. 2B and C), conical shaped teeth, missing mandibular permanent anterior and retained deciduous mandibular canines, and right lateral incisor teeth (Fig. 2C).
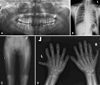
Panoramic radiograph revealed many missing teeth with no impacted tooth (Fig. 3A). Chest radiograph showed homogenous opacity in the left upper zone associated with elevation of hilum and left dome of diaphragm suggestive of left upper lobectomy (Fig. 3B). Antero-posterior view of the legs showed Genu valgum, hypoplasia of lateral end of tibia associated with medial tibial diaphysial outgrowth called exostosis, and mild shortening of fibula (Fig. 3C). Hand-wrist radiograph showed carpal fusion, postaxial polydactyly, and shortening of metacarpal and phalangeal bone with cone shaped epiphysis. There was fusion of capitate and hamate on the right hand and hamate and triquadral on the left hand (Fig. 3D).
A team work of pedodontist, oral and maxillofacial surgeon, and prosthodontist was required to correct the craniofacial and dental defects in this patient. Therefore, the patient was referred to these specialists for further treatment. Conical teeth were built up by composites in Department of Pedodontics. Since the patient was in growing phase, the prosthodontist decided to give acrylic partial dentures for the missing teeth. Oral and maxillofacial surgeon performed frenectomy for the high labial frenum as it was hindering the placement of the partial denture. Patient was on regular follow up.
Discussion
Ellis-van Creveld syndrome (EVC) otherwise known as chondroectodermal dysplasia has autosomal recessive inheritance. It is a syndrome found in Amish population of Pennsylvania in USA, affecting male and female equally.2 Familial history may include parental consanguinity or affected siblings or family members. Our patient was the second child of non-consanguineous and normally developed parents, however her elder sibling had died of similar medical problem.
About 60% of the cases have congenital heart defect. These patients die due to either cardiac problem or respiratory distress.2 Our case did not have any cardiac problem, however there was congenital lobar emphysema because of her dyspnoea. She had undergone left upper lobectomy for the same reason when she was one and half year old child.
The syndrome affects mainly the bones such as the lower limb with genu valgum, which requires surgical correction. The upper limbs show the characteristic bilateral postaxial polydactyly.3,4 Our case had all these limb anomalies.
Other ectodermal features in this syndrome are the absence or hypoplastic features of finger and toe nails, natal teeth, conical shaped or missing teeth, and absence of labial vestibule because of fusion of upper lip to the gingival margin, leading to the notching of upper lip. This could be due to the continuation of the normal serrated condition of the gingiva from the third to seventh month in the uterine life of the fetus. It is considered as the characteristic and diagnostic feature of this syndrome.5-7 All of these features were also present in this case.
This condition can be diagnosed on intrauterine ultrasonographic image. Genetic testing is also useful in diagnosis. There are about 40 independent EVC/EVC2 mutations.8 Ruiz-Perez and Goodship mentioned that the abnormalities in EVC syndrome resulted from the tissue specific disruption of the response to Hh ligands.9
Weyer's syndrome, asphyxiating thoracic dystrophy, and orofacial digital syndrome should be considered in the differential diagnosis of this syndrome. EVC syndrome and Weyer's acrodental dysastosis are allelic conditions caused by loss of function mutation in EVC and EVC2. These are separated by 2-6 kb of genomeric sequence on chromosome 4p16.10 All the features are similar in both conditions except for the fact that there is delay in fusion of mandibular symphysis in acrodental dysastosis.6
Patients with EVC syndrome and asphyxiating thoracic dystrophy will have identical features in hand, pelvis, and long bones. Therefore, it is not possible to differentiate these two conditions radiographically. Presence of cardiac anomalies, nail hypoplasia, fusion of upper lip to gingiva and neonatal teeth in EVC syndrome, and renal failure with hypertension in asphyxiating thoracic dystrophy will help in distinguishing these two disorders from each other.6,11
Presence of multiple gingivolabial frenula is similar to EVC in orofacial digital syndrome. However, it has dominant sex linked inheritance. It is commonly found in women. Hypoplastic nasal cartilage, moderate mental retardation, fissured tongue, and ankyloglossia helps to differentiate this from EVC syndrome.11
In conclusion, the effective management of this syndrome will require a team which includes pedodontist, oral and maxillofacial surgeon, prosthodontist, clinical geneticist, cardiologist, pulmonologist, orthopaedician, urologist, psychologist, pediatrician, and pediatric neurologist. Since the oral manifestation is one of the characteristic diagnostic features, and it affects the esthetic problem, speech, jaw growth of the child, the dentists have an important role to play in proper management of such cases.


 XML Download
XML Download