

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Approximately 15% of couples with a normal sexual life who do not use contraception suffer from infertility, and the prevalence of this condition is insidiously increasing [1]. More than 90% of cases of male factor infertility are characterized by a low sperm count, the production of poor-quality sperm, or a combination thereof, resulting from anatomical problems, hormonal imbalances, and genetic defects [23]. Nevertheless, the etiology and pathogenesis of idiopathic male infertility are still not fully understood [4].
Currently, empirical treatments with various pharmaceutical and herbal agents have been used not only for idiopathic male infertility, but also to enhance the success rates of surgical treatment and in vitro fertilization [56]. The administration of herbs as an infertility treatment has become popular, despite a lack of scientific evidence regarding their effectiveness and safety [7]. Therefore, researchers have continued efforts to develop evidence-based interventions to enhance spermatogenesis in patients with male infertility.
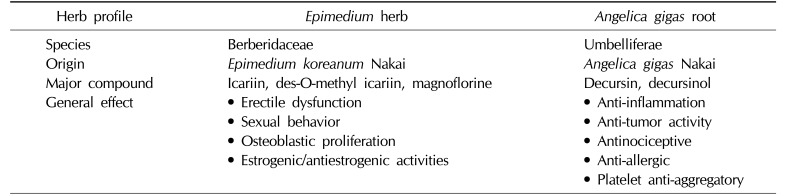
Angelica gigas Nakai is known to exert anticancer and neuroprotective effects through apoptosis, but has also been reported to inhibit fat accumulation and to reduce adipocytokine secretion [89]. In addition, decursin, a major active component of Angelica gigas Nakai, has demonstrated a cellular antioxidant defense capacity through free radical scavenging activity in cryptorchidism-induced male infertility [1011]. Icariin, contained in Epimedium koreanum Nakai, has shown some antioxidant effects, including a reduction of free radicals and lipid peroxidation inhibition [12], and has been found to improve erectile function in aged rats [13]. These results suggest that these herbal compounds have a safe and positive influence on sperm quality and on sexual behavior. However, the effects and mechanisms underlying the combined action of these herbal formulations have not been clearly elucidated in a male infertility model.
In this study, we investigated the endocrine-evoked and antioxidant effects of a new combined herbal formula, KH-465, as a spermatogenesis enhancer in an luteinizing hormone-releasing hormone (LHRH) agonist-induced spermatogenic failure rat model.
MATERIALS AND METHODS
1. Plant material and preparation of the herbal formula
The herbs were purchased from Globalherb Inc. (Andong, Korea). A fresh sample of Angelica gigas Nakai was collected at Bonghwa-gun, Gyeongbuk province, Korea. Epimedium koreanum Nakai was imported from China. The plants were identified by an Oriental medical doctor and phytology expert at the Korea Bio Medical Science Institute Co. Ltd. (Seoul, Korea). The major ingredients in the herbal formula of KH-465 are described in Table 1. Epimedium koreanum Nakai (1,500 g) and Angelica gigas Nakai (1,500 g) were extracted with 12,000 mL of 30% ethanol for 3 hours at 60℃ and 20% ethanol for 4 hours at 60℃, respectively. The solutions were filtered twice through a 50-µm and a 1-µm filter, and concentrated in a vacuum evaporator (60℃) to 52 degrees Brix and 43 degrees Brix, respectively. The residual solvent in each extract was removed in a spray dryer (SD-1000, EYELA; Tokyo Rikakikai Co., Ltd., Tokyo, Japan) for 48 hours at 60℃ in a vacuum. The resulting powders were mixed at a 6:4 weight ratio and stored in a plastic bag until use. The major peak of KH-465, icariin from Epimedium koreanum Nakai and decursin from Angelica gigas Nakai, were analyzed by high-performance liquid chromatography using a Dionex Ultimate 3000 series dual low-pressure ternary gradient pump (Dionex Softron GmbH, Germering, Germany). Three principal icariin and decursin peaks were detected in the chromatogram by diode array detection at 530 nm.
2. Ethics statement
The animal studies were performed after receiving approval of the Institutional Animal Care and Use Committee (IACUC) in Pusan National University Hospital (IACUC approval No. PNUH-2014-060) and were handled according to Guide for the Care and Use of Laboratory Animals.
3. Animal groups and treatment protocol
Twelve-week-old male Sprague-Dawley rats were divided into 5 groups: a normal control (NC) group, which received an intramuscular injection of normal saline, and experimental groups I, II, III, and IV, which received a subcutaneous injection of an LHRH agonist (leuprolide acetate, Leuplin®; Takeda Pharmaceutical Co., Osaka, Japan) for 4 weeks to induce spermatogenic failure. Group I (control) received oral administration of distilled water once a day. Groups II and III received 200 mg/kg and 400 mg/kg of KH-465 for 4 weeks, respectively. Group IV received testosterone enanthate (Jenasteron®; Jaytech Biogen, Seoul, Korea) for 4 weeks as a positive control. KH-465 was dissolved in distilled water and administered orally through an 8 F red Rob-Nel catheter. The dosage of KH-465 and duration of treatment were selected based on results from a preliminary experimental study (data not shown).
4. Measurement of cauda epididymal sperm count and motility
The cauda epididymides were dissected and washed thoroughly in normal saline. The epididymides were finely minced in normal saline containing 0.5% bovine serum albumin at 37℃. Sperm suspensions were placed on prewarmed glass slides and observed under a light microscope in a Neubauer hemocytometer. Sperm motility was expressed at the percentage of sperm that showed any movement. Three counts per sample were averaged.
5. Measurement of testosterone, free testosterone, luteinizing hormone, and follicle-stimulating hormone
Testosterone (ALPCO, Salem, NH, USA), free testosterone (Cusabio, Wuhan, China), luteinizing hormone (LH) (Enzo, Washington, DC, USA), and follicle-stimulating hormone (FSH) (Cusabio) levels in serum were measured using an enzyme-linked immunosorbent assay (ELISA) kit according to the manufacturer's protocol. Briefly, 96-well plates were coated with primary antibody, and 50 µL of standard, control, or samples was added into each well of the plate and incubated following the manufacturer's instructions. After washing, 100 µL of the enzyme-conjugated solution was added and incubated. After the substrate was added, the maximum colorimetric response was determined. The absorbance of the sample was read at 450 nm.
6. Histological evaluation of spermatogenic cell density
Testicular tissues were quickly excised and then fixed in Bouin's solution (Sigma, Louisville, KY, USA) for 24 hours. The fixed testicular tissues were dehydrated and embedded in paraffin wax, sectioned to a 4 µm thickness with a microtome, stained with H&E, and examined using light microscopy at ×400 magnification. Ten characteristic sites in the seminiferous tubules were selected randomly and spermatogenic cell density was measured.
7. Measurement of oxidative stress markers
Oxidative stress in testicular tissue was assessed quantitatively by measuring superoxide dismutase (SOD) activity and 8-hydroxy-2′-deoxyguanosine (8-OHdG) content. Using the DNeasy Blood & Tissue kit (Qiagen, Valencia, CA, USA), total DNA was extracted from the testes. The 8-OHdG levels were measured with a Highly Sensitive 8-OHdG Check ELISA (Cusabio). After the final color was developed with the addition of 3,3′,5,5′-tetramethylbenzidine, the absorbance of the sample was measured at 450 nm. The tissue sample concentration was calculated from a standard curve and was corrected for the DNA concentration. The level of SOD activity in the tissue was measured using a SOD Assay Kit-WST (MyBiosource, San Diego, CA, USA), monitoring the decrease in the rate of superoxide-mediated reduction of nitroblue tetrazolium at 450 nm using a spectrophotometer. Experiments were performed in triplicate.
8. Statistical analysis
All data were presented as the mean±standard deviation. Data were analyzed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). Data were evaluated using analysis of variance, with group comparisons made using the Student t-test. p-values <0.05 were considered to indicate statistical significance.
RESULTS
1. Body and organ weight
The mean testis and epididymis weights are shown in Table 2. There were no significant differences in the body, testis, or epididymis weight between the NC group and the LHRH agonist-induced infertility groups.
2. Effects of KH-465 on sperm parameters and sex hormones
The mean sperm concentration and motility in the LHRH agonist-induced infertility control group I were significantly lower than in the NC group. However, administration of KH-465 improved sperm concentration and motility compared with group I. In particular, administration of 400 mg of KH-465 (group III) led to marked improvements compared to the LHRH-agonist control group I. There was a significant decrease in serum levels of testosterone, free testosterone, FSH, and LH in the LHRH agonist-induced infertility group I compared with the NC group. There were no significant differences in sex hormone levels among the experimental groups (Table 3). LH showed a tendency to be higher in groups II and III than in the LHRH-agonist control group I, but this trend was not statistically significant.
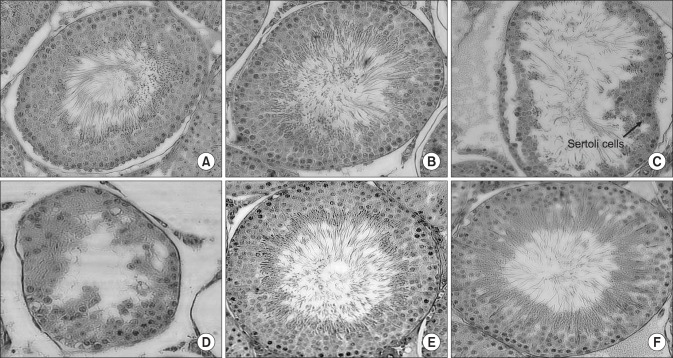
3. Effect of KH-465 on testicular morphology
In the NC group, testicular sections showed small and round seminiferous tubules with a normal arrangement and several layers of spermatocytes forming the germinal cell layer (Fig. 1A). In the samples obtained at 8 weeks, the testicular sections revealed compact and variably sized seminiferous tubules lined by a thick layer of spermatogenic cells in variable stages of maturation, beginning from the primary spermatogonia and extending until final sperm production filled the lumen. The basement membrane of all tubules was thin, with no thickening or peritubular fibrosis (Fig. 1B). In group I, the interstitium was scanty, slightly edematous, and included scattered small groups of Leydig cells with small round monotonous nuclei and prominent tiny nucleoli (Fig. 1C). Upon LHRH induction, in the samples obtained at 8 weeks from group I, a considerable number of spermatocytes showed incomplete spermatogenesis, with arrest at the secondary spermatogenic stage and a reduced number of spermatozoa at the center of the tubules compared with the NC group. The interstitium was edematous, vascular, and congested with normal Leydig cells. Progressive loss of Sertoli cells or arrest at the secondary spermatogenic stage of sperm production was observed in the LHRH-treated groups at 8 weeks (Fig. 1D). However, the most notable morphological changes were observed in group III (treated with KH-465) and group IV (treated with testosterone enanthate). These groups showed complete restoration of normal spermatogenesis in almost all seminiferous tubules, which exhibited satisfactory terminal sperm production by a thick layer of spermatogenic cells in variable stages of maturation and normal Leydig cells (Fig. 1E, 1F).
4. Effects of KH-465 on oxidative stress markers
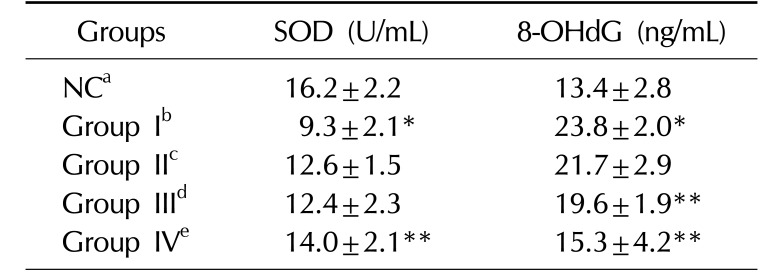
Greater SOD expression was observed in the groups treated with KH-465 than in the LHRH agonist-induced control group I, but this trend was not statistically significant. Less 8-OHdG expression was observed in the group that received 400 mg of KH-465 than in the LHRH agonist-induced control group I (Table 4).
DISCUSSION
The main findings of this study are as follows. Treatment with the new combined herbal formula KH-465, consisting of Epimedium koreanum Nakai and Angelica gigas Nakai, restored sperm count, motility, and spermatogenic cell density, and decreased levels of 8-OHdG and increased levels of SOD in a LHRH agonist-induced infertility rat model. These findings suggest that KH-465 led to the recovery of spermatogenesis and maintenance of normal sperm function in a rat model of infertility.
The acute or chronic treatment of male rats with LHRH or its agonists has been reported to lead to a reduction of testicular weight, the weight of the accessory reproductive glands, testicular LH receptor levels, and plasma testosterone concentration, resulting in suppression of spermatogenesis [1415]. We observed that sperm count, sperm motility, and serum concentrations of testosterone, free testosterone, FSH, and LH in rats with LHRH agonist-induced infertility were significantly lower than the corresponding findings in the NC group. In addition, the spermatogenic cell density in the testes was lower in the LHRH agonist-induced infertility group than in the NC group. Although the mechanism by which the LHRH agonist inhibited spermatogenesis has yet to be determined, LHRH agonists are associated with paradoxical antifertility effects and have been proposed as contraceptive agents for men [14]. In the present study, we found that the LHRH agonist-induced infertility group showed a reduction of endogenous antioxidant enzymes, such as SOD [5].
Several studies have demonstrated that elevated levels of reactive oxygen species (ROS) directly damage sperm DNA and induce apoptosis in sperm [16]. Recently, Bae et al [17] performed an experimental study with ojahwan, investigating the toxicity and influence of this 5-herb mixture on normal reproductive organs. Their results suggest that ojahwan had a safe and positive influence on sperm quality after the oral administration of herbal compounds by decreasing heat shock protein activity and free radical scavenging activity. In the present study, the decreased activity of SOD was improved by KH-465 treatment in rats with LHRH agonist-induced infertility. It is likely that the therapeutic effects of KH-465 are at least in part attributable to suppression of ROS production or free radical scavenging activities, with eventual beneficial effects on sperm function and spermatogenesis. Basic and clinical research has been carried out over the last few decades to explore the effectiveness of herbal medicine in treating male infertility via the improvement of sperm production, sperm quality, and libido, and reductions in oxidative stress [9]. Ginseng expected to be effective in treating male infertility by improving sperm count or motility, and by promoting DNA synthesis or protein metabolism in spermatogenic cells or Sertoli cells of the testes [18].
Although many aspects of the pharmacological mechanisms of natural medicines remain unclear, herbal formulas are already being manufactured and commercialized as various new preparations, including powders, granules, extract balls, and patches. In terms of the underlying molecular mechanisms, some carefully selected herbal extracts are expected to enhance spermatogenesis by exerting a significant influence on the endocrine function of the testes, via antioxidant effects, and by causing improvements in local circulation. Shibahara et al [19] reported that administration of bojungykki-tang significantly improved sperm concentration and sperm motility or fertilizing ability in 16 (69.6%) of 23 male patients with infertility. Takayama et al [20] reported an improvement of sperm count and sperm motility after administration of woochahyunki-hwan in 34 patients with idiopathic infertility, as well as successful pregnancy in patients with oligospermia (33.3%) and asthenozoospermia (14.3%).
Our previous study reported that decursin acted to improve sperm count and motility by increasing antioxidant activity and decreasing apoptosis in patients with male infertility [12]. Li et al [11] reported that decursin may be able to prevent chemotherapy-induced cytotoxicity via the activation of antioxidant enzymes. Chen et al [21] reported that icariin was involved in testosterone production via the regulation of the expression of genes such as peripheral type benzodiazepine receptor and steroidogenic acute regulatory protein, resulting in an improved antioxidant capacity. Icariin also has testosterone mimetic properties, suggesting that it may have therapeutic potential in the management of hypogonadism and erectile dysfunction [22]. In this regard, the effects of KH-465 are at least in part attributable to improvements in sperm count and motility following a reduction of ROS production. Because oxidative stress can cause abnormalities in sperm morphology, motility, concentration, and DNA integrity, attaining an appropriate balance between free radicals and antioxidants is necessary for improving the chances of pregnancy in couples affected by male infertility [23].
This study suggests that the new combined herbal formula KH-465 can be considered as a medication for improving spermatogenesis in patients with idiopathic infertility, since it restored the endocrine regulation of the testes and exhibited a free radical scavenging effect.
One limitation of this study is that it did not identify the exact mechanism of the effects of KH-465 or characterize gene expression in the testes. Another limitation is that the present study did not examine the effect of KH-465 on testicular tissue apoptosis. Further work should investigate the effects of KH-465 on the expression of genes related to antioxidant activity and spermatogenesis in detail. Additional studies are warranted to further investigate KH-465 in terms of endocrinology, cellular immunology, effects on apoptosis, and regulatory functions.
CONCLUSIONS
Our results indicate that the new combined herbal formula KH-465 increases sperm count and motility in rat model of male infertility. The present study suggests that KH-465 is a supplemental agent that may improve the spermatogenesis by reducing oxidative stress in a LHRH agonist-induced infertility.


 XML Download
XML Download