

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Hydatidiform mole with coexistent fetus is very rare, arising about 1 in 20,000 to 100,000 pregnancies. There are limited data to guide the management and treatment. Also it is a dilemma to decide continuation or termination of pregnancy. We experienced a case of hydatidiform mole with a coexistent fetus which was diagnosed with magnetic resonance imaging in a woman of 13th weeks of pregnancy. After termination of pregnancy, the patient treated with prophylactic chemotherapy. We report the case with a brief review of literature.
Figures and Tables
Fig. 1
Transavaginal ultrasound imaging demonstrates multicystic hyperechoic mass (arrow) with coexistent living fetus (arrow head).
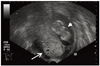
Fig. 2
Magnetic resonance imaging demonstrates normal fetus (thin arrow) of 13 weeks of pregnancy with anterior wall placenta at the right upper portion of uterus, and multiloculated cystic mass (thick arrow) with high signal intensity on T2-weighted image at the left inferior portion of the uterine cavity. (A, B) Sagittal images. (C) Coronal image. (D) Axial image.


References
1. Steller MA, Genest DR, Bernstein MR, Lage JM, Goldstein DP, Berkowitz RS. Natural history of twin pregnancy with complete hydatidiform mole and coexisting fetus. Obstet Gynecol. 1994. 83:35–42.
2. Novick MK, Dillon EH, Epstein NF. AJR teaching file: pregnant woman with vaginal spotting, nausea, and vomiting. AJR Am J Roentgenol. 2010. 194:S79–S82.
3. Wee L, Jauniaux E. Prenatal diagnosis and management of twin pregnancies complicated by a co-existing molar pregnancy. Prenat Diagn. 2005. 25:772–776.
4. Smith HO, Wiggins C, Verschraegen CF, Cole LW, Greene HM, Muller CY, et al. Changing trends in gestational trophoblastic disease. J Reprod Med. 2006. 51:777–784.
5. Kim SJ, Lee C, Kwon SY, Na YJ, Oh YK, Kim CJ. Studying changes in the incidence, diagnosis and management of GTD: the South Korean model. J Reprod Med. 2004. 49:643–654.
6. Vejerslev LO. Clinical management and diagnostic possibilities in hydatidiform mole with coexistent fetus. Obstet Gynecol Surv. 1991. 46:577–588.
7. Niemann I, Petersen LK, Hansen ES, Sunde L. Predictors of low risk of persistent trophoblastic disease in molar pregnancies. Obstet Gynecol. 2006. 107:1006–1011.
8. Sebire NJ, Foskett M, Paradinas FJ, Fisher RA, Francis RJ, Short D, et al. Outcome of twin pregnancies with complete hydatidiform mole and healthy co-twin. Lancet. 2002. 359:2165–2166.
9. Garner EI, Goldstein DP, Feltmate CM, Berkowitz RS. Gestational trophoblastic disease. Clin Obstet Gynecol. 2007. 50:112–122.
10. Menczer J, Modan M, Serr DM. Prospective follow-up of patients with hydatidiform mole. Obstet Gynecol. 1980. 55:346–349.
11. Fowler DJ, Lindsay I, Seckl MJ, Sebire NJ. Routine pre-evacuation ultrasound diagnosis of hydatidiform mole: experience of more than 1000 cases from a regional referral center. Ultrasound Obstet Gynecol. 2006. 27:56–60.
12. Shellock FG, Kanal E. SMRI Safety Committee. Policies, guidelines, and recommendations for MR imaging safety and patient management. J Magn Reson Imaging. 1991. 1:97–101.
13. Wu TC, Shen SH, Chang SP, Chang CY, Guo WY. Magnetic resonance experience of a twin pregnancy with a normal fetus and hydatidiform mole: a case report. J Comput Assist Tomogr. 2005. 29:415–417.
 XML Download
XML Download