

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Few cases of pulmonary barotrauma after self-contained underwater breathing apparatus (SCUBA) diving have been reported, but little is known about pulmonary barotrauma associated with snorkeling. We report a rare case of a pulmonary complication of hemoptysis associated with pulmonary alveolar hemorrhage, a possible complication of snorkeling. Complete recovery was observed within few days.
CASE REPORT
A healthy 54-year-old man with hemoptysis and a previous medical history of well-controlled hypertension (body weight, 74.5 kg; height, 168 cm; body mass index, 26.14 kg/m2) visited our hospital. He reported with approximately 20–30 mL of expectorated blood mixed with sputum. He had been well before the current attack. This was not his first attempt at snorkeling, and he had more than 5 years of snorkeling experience. He snorkeled about twice a year without any problems, and this was the first attack he had experienced. Several hours before admission, he had been snorkeling in the late afternoon at a river for 1 hour, without any traumatic injury to his chest. After snorkeling, he noticed blood-tinged sputum while coughing. He denied any accompanying aspiration of water or other respiratory symptoms, including shortness of breath. He presented to the emergency department of our hospital with a pulse rate of 90 beats per minute and respiratory rate of 20 breaths per minute. His body temperature was within normal range, with no chills or other upper respiratory symptoms. Although he was fully conscious and lucid, he appeared to be acutely ill. Hemoptysis was his only complaint, and there were no other symptoms. His breath sounds were normal, without any crackle or abnormal sounds.
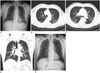
On admission, he underwent laboratory testing for any possible infection. There was no evidence of definite leukocytosis or inflammation, and his normal hemoglobin level and coagulation functions were normal. Initial chest X-ray revealed diffuse bilateral ground-glass opacity (GGO) and multifocal patchy consolidation in both lung zones, suggesting a pulmonary hemorrhage or edema component (Fig. 1A). For further evaluation of this lesion, he underwent chest computed tomography (CT). Chest CT reported similar findings of patchy GGOs mixed with smooth interlobular septal thickening in all 5 lobes bilaterally, mainly located in the dependent portion of both upper lobes. There was no remarkable zonal predominancy or abnormal findings in the large airways (Fig. 1B-D). No pleural effusion or pneumothorax were observed. We speculated that he had a pulmonary alveolar hemorrhage mixed with a pulmonary edema component, associated with barotrauma after snorkeling.
To prevent further possible bleeding, tranexamic acid was administered to the patient for the first 3 days. Follow-up chest X-ray on the second hospital day revealed marked clearing of the previously noted GGOs in both lungs (Fig. 1E). Bronchoscopy was attempted on the third hospital day, but it failed due to low compliance from the patient. On the fourth hospital day, the clinical features were stable, and therefore the patient was discharged. Follow-up bronchoscopy and chest CT were not performed.
DISCUSSION
We present an extraordinary case of a middle aged man with pulmonary alveolar hemorrhage caused by pulmonary pressure injury after snorkeling, without any other underlying pulmonary disease. Chest X-ray and chest CT findings showed a patchy GGO appearance in the dependent portions of both upper lobes and along the bronchovascular bundles, suggesting alveolar hemorrhage mixed with a pulmonary edema component.
In previous literature regarding alveolar hemorrhage as a complication of barotrauma caused by SCUBA diving, the increase in the intra-alveolar pressure due to breath holding in the water and the mechanism of barotrauma, which induced intra-alveolar hemorrhage, appeared to be similar to those seen in our case. During breath holding while swimming (including snorkeling), immersion in a reversed position causes a pressure difference between the thorax and lower extremities. Additionally, the coldness induced by water increases this hemodynamic strain (12). The pressure difference causes blood circulation from the peripheral portion (extremities) to the central portion of the body (heart, lungs, and great vessels of the chest) and enlarges the venous return and cardiac preload (34). Relative pulmonary hypertension leads to an increased pressure gradient between the pulmonary capillaries and pulmonary parenchyma. Also, in case of head-out water immersion, alveolar pressure is similar to atmospheric pressure, whereas extra-thoracic vascular pressure is similar to hydrostatic pressure. These differences make the blood mass transfer toward the thorax, and results in pulmonary hypertension and consequent pulmonary barotraumas (5). The pressure in the capillaries exceeds the intra-alveolar pressure, resulting in leakage of fluid or blood into the lungs and contributing to the pulmonary edema or pulmonary hemorrhage (3678)
SCUBA and snorkeling share a similar mechanism in barotrauma, but they also have some differences. In case of SCUBA, the breathing gas is sucked through the regulator and enters the lungs with the same pressure as the ambient pressure. Sudden head-out elevation in water decreases the ambient pressure and causes the pressure of the breathing gas to be higher than the ambient pressure, resulting in pulmonary barotraumas. In contrast, in case of head-out water immersion in snorkeling, the diver suffers breath and the pressure in the alveoli equivalent to the ambient pressure. Even in case of a sudden rise, the pressure in the alveoli and the ambient pressure are maintained at the same level. This difference causes the barotraumas, and is more common in SCUBA.
Pulmonary alveolar hemorrhage is a very rare but important manifestation of barotrauma, in swimmers who engage in breath holding or snorkeling (9). Since our patient had engaged in snorkeling with intermittent breath holding for ≥ 1 hour, barotrauma from the reversed position of the chest to the lower extremities, and blood mass transfer to the thorax because of pressure difference between alveoli and extra-thoracic vessels, are the most reliable cause of pulmonary alveolar hemorrhage. Although there has been a case report about barotrauma-related pulmonary hemorrhage after SCUBA diving, to our knowledge, this is the first case report concerning transient pulmonary alveolar hemorrhage after snorkeling in Korea (67). Pulmonary alveolar hemorrhage was the main clinical manifestation associated with snorkeling in this patient. Radiologists and clinicians may encounter patients with alveolar hemorrhage as a manifestation of barotrauma.
 XML Download
XML Download