

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To investigate the frequency of vesicoureteral reflux (VUR) in children with renal anomalies aevaluate the correlation between renal anomalies and VUR.
Materials and Methods
Eighty-one children (1 day-8 years) with renalanomalies underwent voiding cystourethrogram between 2006 and 2009 were reviewed. This study included ureteropelvic junction stenosis (n = 32), ureteropelvic duplication (n = 20), multicystic dysplastic kidney (n = 12), fusion anomaly (n = 11), renal agenesis (n = 3), unilateral renal hypoplasia (n = 2), and ectopic kidney (n = 1). The frequency, grade, and location of VUR were evaluated. The grade of VUR according to age and anomaly type was statistically analyzed, and the patients with VUR were followed.
Results
The VUR was present in 14 (17.3%); ipsilateral VUR was present in 8 (57.1%), bilateral VUR in 4 (28.6%), and contralateral VUR in 2 (14.2%). VUR was detected in 9 patients under the age of one. There was no statistical correlation between VUR grade and either age or anomaly type of the nine patients showed continuous VUR on up.
Figures and Tables
Fig. 1
Congenital renal hypoplasia of the right kidney with right vesicoureteral reflux grade 4 in a 1-month-old boy.
A. Anterior view of the Tc-99 m-DMSA renal scan shows decreased activity of right kidney (arrow).
B. Voiding cystourethrography shows the grade 4 vesicoureteral reflux in the right kidney.
Note.-DMSA = dimercaptosuccinic acid
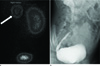
Fig. 2
A neonate with right multicystic dysplastic kidney and left vesicoureteral reflux grade 1.
A. Coronal reconstructed CT image shows several cysts in right renal fossa (arrowhead).
B. Voiding cystourethrography after 4 days reveals grade 1 vesicoureteral reflux (arrow) in contralateral kidney.
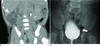
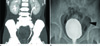
Fig. 3
A 8-year-old girl with bilateral ureteropelvic duplication and left vesicoureteral reflux grade 1.
A. Coronal MIP CT image shows duplication of both collecting system.
B. Voiding cystourethrography after 1 month demonstrates grade 1 left vesicoureteral reflux (arrowhead).
Note.-MIP = Maximum Intensity Projection


References
1. Lee WH, Kim YT, Jo SS, Kim SW, Shin HC, Kim IY. Clinical significance of renal pelvic dilatation less than 10 mm in neonates: correlation with urinary tract infection and vesicoureteral reflux. J Korean Soc Radiol. 2009; 61:429–433.
2. Kim DW, Lim IS, Choi ES. The decision of voiding cystourethrography in children with urinary tract infection. J Korean Soc Pediatr Nephrol. 2007; 11:203–211.
3. Wilson C, Azmy AF. Horseshoe kidney in children. Br J Urol. 1986; 58:361–363.
4. Ben-Ami T, Sinai L, Hertz M, Boichis H. Vesicoureteral reflux in boys: review of 196 cases. Radiology. 1989; 173:681–684.
5. Cascio S, Sweeney B, Granata C, Piaggio G, Jasonni V, Puri P. Vesicoureteral reflux and ureteropelvic junction obstruction in children with horseshoe kidney: treatment and outcome. J Urol. 2002; 167:2566–2568.
6. Fernbach SK, Feinstein KA, Spencer K, Lindstrom CA. Ureteral duplication and its complications. Radiographics. 1997; 17:109–127.
7. Krzemień G, Roszkowska-Blaim M, Kostro I, Wojnar J, Karpińska M, Sekowska R. Urological anomalies in children with renal agenesis or multicystic dysplastic kidney. J Appl Genet. 2006; 47:171–176.
8. van den Bosch CM, van Wijk JA, Beckers GM, van der Horst HJ, Schreuder MF, Bökenkamp A. Urological and nephrological findings of renal ectopia. J Urol. 2010; 183:1574–1578.
9. Bomalaski MD, Hirschl RB, Bloom DA. Vesicoureteral reflux and ureteropelvic junction obstruction: association, treatment options and outcome. J Urol. 1997; 157:969–974.
10. Klare B, Geiselhardt B, Wesch H, Schärer K, Immich H, Willich E. Radiological kidney size in childhood. Pediatr Radiol. 1980; 9:153–160.
11. Medical versus surgical treatment of primary vesicoureteral reflux: a prospective international reflux study in children. J Urol. 1981; 125:277–283.
12. Risdon RA, Young LW, Chrispin AR. Renal hypoplasia and dysplasia: a radiological and pathological correlation. Pediatr Radiol. 1975; 3:213–225.
13. Oliveira EA, Diniz JS, Silva JM, Rabelo EA, Pontes AK, Souza MF. Features of primary vesicoureteric reflux detected by investigation of foetal hydronephrosis. Int Urol Nephrol. 1998; 30:535–541.
14. Risdon RA. The small scarred kidney in childhood. Pediatr Nephrol. 1993; 7:361–364.
 XML Download
XML Download