

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
A dyshormonogenetic goiter is a congenital hyperplasia of the thyroid parenchyma caused by a defect in the noraml hormongenetic pathway. Here, we report on a case involving the simultaneous occurrence of a thyroid and an ectopic thyroid dyshormonogenetic goiter. We describe the ultrasound and CT findings along with a brief literature review.
Figures and Tables
Fig. 1
Neck CT and ultrasonography of goiter and left neck mass in 45-year-old female.
A. Axial image of non-contrast enhanced CT shows low attenuated thyroid gland and left neck mass with high attenuated portions (arrow) and small calcifications.
B. Axial image of contrast enhanced CT shows heterogenous enhancements in thyroid gland and left neck mass with non-enhancing foci (arrow).
C. Ultrasonographic finding shows heterogenous isoechoic mass in left supraclavicular area.
D. Ultrasonographic finding shows a nodular calcification in left thyroid gland.

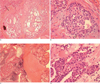
Fig. 2
Microscopic histology of goiter and left neck mass in 45-year-old female.
A. A photomicrograph of goiter shows multiple hyperplastic nodules with fibrotic tissue (black arrow) and calcification (H & E, ×100).
B. A photomicrograph of goiter shows complex microfollicles with atypical nodules in the fibrosis tissue between hyperplastic nodules (H & E, ×400).
C. A photomicrograph of neck mass shows normal thyroid tissue and multiple hyperplastic nodules with fibrotic tissue (H & E, ×100).
D. A photomicrograph of neck mass shows similar microscopic findings with goiter (H & E, ×400).
References
1. Lever EG, Medeiros-Neto GA, DeGroot LJ. Inherited disorders of thyroid metabolism. Endocr Rev. 1983; 4:213–239.
2. Pfarr N, Musholt TJ, Musholt PB, Brzezinska R, Pohlenz J. Congenital primary hypothyroidism with subsequent adenomatous goiter in a Turkish patient caused by a homozygous 10-bp deletion in the thyroid peroxidase (TPO) gene. Clin Endocrinol. 2006; 64:514–518.
3. Fadda G, Baloch ZW, LiVolsi VA. Dyshormonogenetic goiter pathology. Int J Surg Pathol. 1999; 7:125–131.
4. Ljungberg 0. Dyshormonogenetic goiter. Biopsy pathology of the thyroid and parathyroid. London: Chapman and Hall Medical;1992. p. 77–79.
5. LiVolsi VA. Surgical pathology of the thyroid. Philadelphia: W. B. Saunders;1990. p. 174–177.
6. Cooper DS, Axelrod L, DeGroot LJ, Vickery AL Jr, Maloof F. Congenital goiter and the development of metastatic follicular carcinoma with evidence for a leak of nonhormonal iodide. Clinical, pathological, kinetic, and biochemical studies and a review of the literature. J Clin Endocrinol Metab. 1981; 52:294–230.
7. Medeiros-Neto G, Bunduki V, Tomimori E, Gomes S, Knobel M, Martin RT, et al. Prenatal diagnosis and treatment of dyshormonogenetic fetal goiter due to defective thyroglobulin synthesis. J Clin Endocrinol Metab. 1997; 82:4239–4242.
8. Baris I, Arisoy AE, Smith A, Agostini M, Mitchell CS, Park SM, et al. A novel missense mutation in human TTF-2 (FKHL15) gene associated with congenital hypothyroidism but not athyreosis. J Clin Endocrinol Metab. 2006; 91:4183–4187.
9. Caccetta TP, Kumar A, Ishak H. Lateral aberrant thyroid tissue presenting as a lateral neck mass. ANZ J Surg. 2005; 75:1123–1124.
10. Gordon B, Yaakob W, Willi S, Buse M, Gordon L. Congenital thyroid disease revisited: migrational anomalies and dyshormonogenesis. J Nucl Med Technol. 1999; 27:282–286.
 XML Download
XML Download