

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Objective
It is still unclear to predict the postoperative drainage volume of chronic subdural hematoma (CSDH) and the relation between the degree of brain shifting and the postoperative drainage volume, even CSDH is relatively common disease. In this study, the authors evaluate the relationship between the brain shifting index and the postoperative drainage volume, and investigated the influencing factors associated with the postoperative drainage volume in CSDH.
Methods
Fifty-eight CSDH with 45 patients, who were operated from November 2003 to April 2006, were enrolled. We investigated multiple factors associated with CSDH including the hemorrhage density and measured the parameters about the brain compliance on computed tomography (CT) as it followed (A, the distance between both inner skull table at the level of frontal horn of lateral ventricle; B, the distance between the most medial side of caudate nucleus head and the ipsilateral inner skull table at the same level of the parameter A; C, the distance of midline shifting at the level of third ventricle; D, the largest thickness of chronic subdural hematoma). We estimated the brain shifting index using the degree of frontal horn compression and midline shifting by the B/A or C/D ratios and the statistical analysis for the relation with the postoperative drainage volume was done.
Results
The mean age was 63.8±25.2 years and mean drainage volume was about 248.8±173.2 mL. Mean drainage date was 5.9±1.5 days and the daily drainage volumes were 109.5, 50.9, 22.2, 14.4, 15.8 mL respectively. The postoperative drainage volume of CSDH was significant correlated with the density of CSDH in brain CT (p=0.04), and the postoperative drainage volume was decreased as the B/A ratio increased (r=0.299, p=0.023).
Figures and Tables
FIGURE 1
Parameters to estimate the brain shifting index of CSDH. A: The distance between both inner skull table at the level of frontal horn of lateral ventricle. B: The distance between most medial side of caudate nucleus head and the ipsilateral inner skull table at the same level of the parameter A. C: The distance of midline shifting at the level of third ventricle. D: The largest thickness of chronic subdural hematoma. CSDH: chronic subdural hematoma.
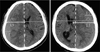
FIGURE 2
The relation between the B/A ratio, brain shifting index, and the postoperative drainage volume of CSDH. Using the regression analysis, the correlation coefficient was 0.29915, and the line of tendency was checked as 'Postoperative drainage volume=-904.3×B/A ratio+757.4' (p-value=0.022538). This means that the postoperative drainage volume increase as the brain shifting index B/A ratio decreased. B/A: the ratio of the distance between the most medial side of caudate nucleus head and the ipsilateral inner skull table (B) over the distance between both inner skull table at the level of frontal horn of lateral ventricle at the same level (A), CSDH: chronic subdural hematoma.
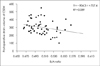
FIGURE 3
The relation between the C/D ratio, brain shifting index, and the postoperative drainage volume of CSDH. Using the regression analysis, the correlation coefficient was 0.164047, and the line of tendency was checked as 'Postoperative drainage volume=-123.2×C/D ratio+359.9' (p-value=0.218509). This means that the postoperative drainage volume was not correlated with the brain shifting index C/D ration in statistic analysis. C/D: the ration of the distance of midline shifting at the level of third ventricle (C) over the largest thickness of chronic subdural hematoma (D), CSDH: chronic subdural hematoma.
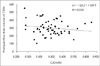
FIGURE 4
The comparison of the B/A and C/D ratios, brain shifting indexes, on brain CT imaging on the basis of drainage volume (200 mL) of CSDH. The B/A and C/D ratios, brain shifting indexes, on brain CT imaging on the basis of 200 mL CSDH drainage volume was shown (p<0.05). The brain shifting index B/A ratio is 0.5202 in the drainage volume lesser than 200 mL and it was decreased to 0.4932 in the drainage volume more than 200 mL. Also the brain shifting index C/D ratio was decreased from 0.5652 to 0.4932 as the drainage volume was increased from the lesser than 200 mL to the more than 200 mL. CSDH: chronic subdural hematoma, B/A: the ratio of the distance between the most medial side of caudate nucleus head and the ipsilateral inner skull table (B) over the distance between both inner skull table at the level of frontal horn of lateral ventricle at the same level (A). C/D: the ration of the distance of midline shifting at the level of third ventricle (C) over the largest thickness of chronic subdural hematoma (D).

TABLE 1
Summary of risk factors in 45 patients with chronic subdural hematoma

*statistically significant difference, †statistically some difference. ns: non-specific, B/A: the ratio of the distance between the most medial side of caudate nucleus head and the ipsilateral inner skull table (B) over the distance between both inner skull table at the level of frontal horn of lateral ventricle at the same level (A), C/D: the ration of the distance of midline shifting at the level of third ventricle (C) over the largest thickness of chronic subdural hematoma (D), DM: diabetic mellitus

References
1. Cameron MM. Chronic subdural hematoma: a review of 114 cases. J Neurol Neurosurg Psychiatry. 1978; 41:834–839.
2. French BN, Cobb CA, Corkill G, Youmans JR. Delayed evolution of post-traumatic subdural hygroma. Surg Neurol. 1978; 9:145–148.
3. Friede RL, Schachenmayr W. The origin of subdural neomembranes. II. Fine structural of neomembranes. Am J Pathol. 1978; 92:69–84.
4. Fujisawa H, Ito H, Saito K, Ikeda K, Nitta H, Yamashita H. Immunohistochemical localization of tissue-type plasminogen activator in the lining wall of chronic subdural hematoma. Surg Neurol. 1991; 35:441–445.

5. Gardner WJ. Traumatic subdural hematoma with particular reference to the latent interval. Arch Neurol Psychiat. 1982; 27:847–858.
6. Hamilton MG, Frizzel JB, Tranmer BI. Chronic subdural hematoma: the role for craniotomy reevaluated. Neurosurgery. 1993; 33:67–72.
7. Kasner SE. Geometry and subdural hematoma volume. Stroke. 1999; 30:188.
8. Tsutsumi K, Maeda K, Iijima A, Usui M, Okada Y, Kirino T. The relationship of preoperative magnetic resornance imaging findings and closed system drainage in the recurrence of chronic subdural hematoma. J Neurosurg. 1997; 87:870–875.
9. Kwon TH, Park YK, Lim DJ, Cho TH, Chung YG, Chung HS, et al. Chronic subdural hematoma: evaluation of the clinical significance of postoperative drainage volume. J Neurosurg. 2000; 93:796–799.
10. Lee SC, Kang JK, Jung HT, Dho JO. Factors affecting brain re-expansion after simple burr hole drainage in chronic subdural hematoma. J Korean Neurosurg Soc. 1998; 27:757–762.
11. Lim DJ, Park YK, Chung YG. The relationship of preoperative computerized tomographic scan image and amount of prospective closed system drainge in the recurrence of chronic subdural hematoma. J Korean Neurosurg Soc. 1998; 27:1402–1407.
12. Laumer R, Schramm J, Leykauf K. Implantation of a reservoir for recurrent subdural hematoma drainage. Neurosurgery. 1989; 25:991–996.
13. Markwalder TM, Seiler RW. Chronic subdural hematomas: to drain or not to drain? Neurosurgery. 1985; 16:185–188.
14. Markwalder TM, Steinsiege KF, Rohner M, Reichenbach W, Markwalder H. The course of chronic subdural hematomas after burrhole craniostomy and closed system drainage. J Neurosurg. 1981; 55:390–396.
15. Nomura S, Kashiwagi S, Fujisawa H, Ito H, Nakamura K. Characterization of local hyperfibrinolysis in chronic subdural hematomas by SDS-PAGE and immunoblot. J Neurosurg. 1994; 81:910–913.
16. Ohno K, Suzuki R, Masaoka H, Matsushima Y, Inaba Y, Monma S. Chronic subdural hematoma proceeded by persistent traumatic subdural fluid collection. J Neurol Neurosurg Psychiatry. 1987; 50:1694–1697.
17. Petersen OF, Espersen JO. Extradural hematomas: measurement of size by volume summation on CT scanning. Neuroradiology. 1984; 26:363–367.
18. Sato S, Suzuki J. Ultrastructural observation of the capsule of chronic subdural hematoma in various clinical stages. J Neurosurg. 1975; 43:569–578.
19. Schachenmayr W, Friede RL. The origin of subdural neomembranes. I. Fine structure of the dura-arachnoid interface in man. Am J Pathol. 1978; 92:53–68.
20. Shim YS, Park CO, Hyun DK. What are the causative factors for a slow, progressive enlargement of a chronic subdural hematoma? Yonsei Med J. 2007; 48:210–217.
21. Sucu HK, Gokmen M, Gelal F. The value of XYZ/2 technique compared with computer-assisted volumetric analysis to estimate the volume of chronic subdural hematoma. Stroke. 2005; 36:998–1000.
22. Tabaddor K, Shulman K. Definite treatment of chronic subdural hematoma by twist-drill craniostomy and closed-system drainage. J Neurosurg. 1977; 46:220–226.
23. Wakai S, Hashimoto K, Watanabe N, Inoh S, Ochiai C, Nagai M. Efficacy of closed-system drainage in treating chronic subdural hematoma: a prospective comparative study. Neurosurgery. 1990; 26:771–773.
24. Yamashima T, Yamamoto S. How do vessels proliferate in the capsule of a chronic subdural hematoma? Neurosurgery. 1984; 15:672–678.
 XML Download
XML Download