

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Actinomycosis is an uncommon, indolent, slowly progressive infection caused by anaerobic or microaerophilic bacteria that normally colonize the mouth, colon, and vagina [1]. Actinomycosis occurs rarely in humans, but occurs more frequently in cattle as a disease called lumpy jaw [2]. It often presents as a slowly progressive, indolent, indurated infiltration with multiple abscesses, fistulas, and sinuses [3]. Four clinical forms of actinomycosis account for most of these human infections: the cervicofacial, thoracic, abdominopelvic, and cerebral [4].
Actinomyces exist in normal oral flora, and they can be found in calculus, periodontal pockets, carious lesions, and oral mucosal surfaces [4]. The bacteria do not cause any pathology as long as they stay on the surface of the mucosa, but they become pathogenic and can initiate a prolonged chronic inflammatory process if the integrity of the mucosal barrier is compromised and access to the oral tissues or jawbones is gained [3].
Actinomycosis of the jaws and oral tissues has been considered for a long time to be a rare disease; therefore, it has not generated much interest in research [4]. Actinomycosis is reported to be very rare in daily dental practice [5]. Other types of actinomycosis in oral tissues, such as periapical actinomycosis, are relatively well documented in the literature, but reports of actinomycosis with clinical and radiographic findings similar to periodontitis are limited [6]. One case has been reported of a regional alveolar bone actinomycosis with a related juvenile-periodontitis-like lesion [7].
A patient was diagnosed with actinomycosis without abscess formation or desquamation based on a biopsy during a periodontal flap procedure. The clinical and radiographic manifestations of actinomycosis were clinically indistinguishable from periodontitis. This article reports a case of actinomycosis-mimicking periodontitis, and provides a review of the literature related to actinomycosis.
CASE REPORT
A 46-year-old female was referred to the Department of Periodontics of Seoul St. Mary's Hospital (Seoul, Korea) for treatment of chronic periodontitis, particularly in the mandibular molar area (Fig. 1). She complained of throbbing pain on the right first and second molars of the mandible. The pain lasted three days. The patient's medical and dental histories were taken, and clinical assessments and examination, including probing depths, tooth mobility, and bleeding on probing, were performed. The patient was a nonsmoker and went to the Department of Cardiology of Seoul St. Mary's Hospital for rheumatic mitral insufficiency; she had been taking an anticoagulant (Warfarin, 2 mg Cuparin tablets; Hana Pharm Co., Seoul, Korea) for 3 years. Intraoral examination revealed generalized chronic periodontitis and particularly deep probing pocket depths: 7 to 8 mm on the distal area of the left second molar, right first molar, and right second molar of the mandible. Her oral hygiene status was relatively good. Her cardiologist was consulted for operability, and the cardiologist recommended continuing anticoagulant therapy.
The initial cause-related therapy consisted of thorough full-mouth scaling and root planing in the quadrants under local anesthesia. This procedure was performed using a combination of hand and ultrasonic instrumentation. The patient received detailed oral hygiene instructions on using a soft toothbrush and floss.
Three weeks after her final root planing treatment, she made an unscheduled visit to the clinic. She complained of recurrence of throbbing pain on the right first molar of the mandible. An intraoral examination was performed to exclude pulpitis or cracked tooth syndrome. There was no swelling, redness, fever, or suppuration. The right first and second molars of the mandible had positive responses for percussion, cold, and electric pulp testing. The possibility of pulpitis or cracked tooth syndrome was ruled out. She complained of an unusual throbbing pain, which was relieved when she bit tightly. The probing pocket depth of the distal area on the right first molar was 7 mm. There was no swelling, redness, fever, or suppuration. The right first and second molars of the mandible had positive responses for percussion, cold, and electric pulp testing. The mobility was within normal range. A periodontal flap procedure was planned to aid in the diagnosis.
Anesthesia was performed using 2% lidocaine containing 1:100,000 epinephrine. A sulcular incision was made around the right posterior teeth of the mandible to preserve the papillae, and the mucoperiosteal buccal and lingual access flaps were elevated (Fig. 2). Granulation tissue adherent to the teeth and the alveolar bone was removed. A round, hard, floating, bluish-gray fragment in the interproximal area between the right first and second molar of the mandible was seen. The remaining area was debrided and irrigated with a saline solution. The resulting interproximal crater defect was filled with a xenograft bone material (Bio-Oss, Geistlich Pharma AG, Wolhusen, Switzerland). The flap was replaced and sutured with nylon 5-0. An analgesic (300 mg acetaminophen, 300 mg Endapen tablet; Chodang Pharm Co., Seoul, Korea) at 3 times a day, and an antimicrobial drug (625 mg amoxicillin with clavulanate, 625 mg Moxicle tablet; Daewoong Co., Seoul, Korea), 3 times a day, were prescribed for 5 days. The patient was also instructed to abstain from brushing and flossing around the surgical area for 2 weeks, to use a 0.1% chlorhexidine (Hexamedine Solution, Bukwang Pharm Co., Seoul, Korea) solution rinse, and to consume a diet of soft food until suture removal. The follow-up visits after the surgical procedure were scheduled for each week of the first month after surgery.
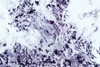
The mass removed from the interproximal alveolar bone was stored in 10% formalin, and was sent to the Department of Pathology of Seoul St. Mary's Hospital for diagnosis. Five days after biopsy, the pathologist concluded that the fragment was aggregates of bacterial colonies and needed a special stain for diagnosis. After one week, the results of the Gram, silver, and periodic acid-Schiff (PAS) stain were positive, and the differential diagnosis was actinomycosis (Figs. 3-6).
Gram positive colonies of actinomyces and inflammatory cell infiltration can be observed (Fig. 4). The actinomycotic aggregate presented an isolated mass of bacterial filaments in the center and periphery, the so-called sun-ray effect (Figs. 4 and 5). The bacterial colonies appeared to be club-shaped. Histologic examination revealed fragments of fibrous tissue containing inflammatory cell infiltrates.
The healing was uneventful, and the patient reported mild discomfort, but was satisfied with the absence of throbbing pain. Based on the histologic result, the patient was prescribed to continue taking amoxicillin and clavulanate (625 mg three times a day for 4 weeks). The patient was monitored weekly for the first month and then monthly for four months. The patient did not report any symptoms, and she is now scheduled for ongoing follow-up.
DISCUSSION
The present study has identified actinomycosis-mimicking periodontal disease without abscesses or fistulas. A previous case reported on an adult patient who presented with periodontitis with a diffuse and atypical actinomycotic lesion that was limited to the gingiva and had an abscess formation, a large desquamation, and subsequent exposure of the alveolar bone in the involved region [8].
Actinomyces colonies can be identified using hematoxylin-eosin, Gram, PAS stains, and silver stain, exhibiting filamentous morphology with color variation between the center and periphery [4]. The colonies have a basophilic center with eosinophilic rays terminating in pear-shaped clubs, the so-called sun-ray effect [9]. In this case, Gram, PAS, and silver stains were performed, and the results were positive.
Infection by Actinomyces may initiate complications, which may not be diagnosed correctly unless the tissue is biopsied and the Actinomyces colonies are identified [4]. In the clinical practice of periodontology, tissue is not routinely submitted for histopathologic analysis [10], and the authors would like to suggest more routine submissions of tissue removed from the oral cavity, especially during the treatment of periodontal disease. Moreover, due to the opportunistic characteristics of the actinomycotic infection, early and adequate differential diagnosis of actinomycosis, prior to attempts at therapy and management steps, is of great importance in the oral cavity because it can prevent the spread of the disease [8].
In a previous report, the majority of cases of actinomycosis were asymptomatic, with only 18% presenting symptoms such as pain and sensory disturbances (80% and 20% of the symptomatic cases, respectively) [4]. In this case, the patient had a recurrence of throbbing pain.
Actinomycotic patients have often been afflicted by more than one medical condition [4]. Won et al. [11] have described actinomycosis as an opportunistic infection, suggesting cancer, immunodeficiency steroids taken over a long period of time, and malnutrition as possible contributing factors. However, most of the actinomycotic patients from the Indian subcontinent have been systemically healthy [10].
Extended antimicrobial therapy has been recommended for patients with any clinical form of actinomycosis to prevent disease recrudescence [9]. However, individualization of therapy is recommended whether the duration of antibiotics depends on the initial burden of disease, the site of infection, or the clinical and radiological response to treatment [12]. Actinomyces are sensitive to a number of antibiotics, and penicillin is the drug of choice for treating an infection caused by any of the Actinomyces [6]. In this report, the combination of penicillin (amoxicillin) and a beta-lactamase inhibitor (clavulanate) are recommended because this offers the advantage of coverage against penicillin-resistant aerobic and anaerobic copathogens [9,11]. The density of Actinomyces colonies, representing the bacterial load in the tissue, may also be considered because the length of antibiotic treatment may be modified according to the density [4]. Surgical excision or debridement may be desired as well, especially if extensive necrotic tissue, fistulas, or a neoplasm is present [6,9]. The patient did not present any recurrence of actinomycosis after a short course of amoxicillin-clavulanate because the infected tissue was totally excised [11].
Actinomycosis should be included in the differential diagnosis in cases where pain has not responded to the appropriate periodontal treatment and the periapical lesion has not been detected. More routine submissions of tissue removed from the oral cavity may be beneficial for differential diagnosis.





 XML Download
XML Download