

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Bisphosphonates (BPs) are drugs for inhibiting bone resorption, widely used for the treatment of osteoporosis, multiple myeloma and skeletal complications of bone metastases. BPs were proven to inhibit decreases in bone density and prevent bone fracture by reducing activation of osteoclasts and inducing apoptosis of osteoclasts. The two main categories of BPs are the non-nitrogen and nitrogen-containing BPs [1,2]. Alendronate is an oral nitrogen-containing BP and the most commonly used drug to treat osteoporosis and osteopenia. Even though BPs have clinical efficacy, a number of cases of osteonecrosis of the jaw involving a patient treated with BPs for a long period of time have been reported worldwide since Marx [3] reported the first case, and this has been recognized as a serious adverse effect of these drugs.
The American Association of Oral and Maxillofacial Surgeons (AAOMS) suggests patients may be considered to have bisphosphonate-related osteonecrosis of the jaw (BRONJ) if each of the following 3 characteristics are present: 1) current or previous treatment with BPs, 2) exposed, necrotic bone in the maxillofacial region that has persisted for more than 8 weeks, and 3) no history of radiation therapy to the jaws [4]. The American Dental Association Council on Scientific Affairs (ADA CSA) reported that the incidence of BRONJ for patients receiving alendronate for a long period of time was estimated to be 0.7 per 100,000 person years of exposure [5]. Even though BRONJ occurs infrequently, risk factors such as systemic/local factors, potency of BPs and period of taking BPs may raise the incidence rate of BRONJ [6]. Recently, implant treatment cases have increased markedly. Furthermore, as the population ages, the numbers of patients who have been treated with BPs or continue to use them for treatment of osteoporosis is on the rise. As a result, the risk of BRONJ for patients who are receiving BPs is increasing after implant placement.
This case report illustrates a 67-year-old female patient who had received oral BPs and developed a significant bone defect with necrosis after proper implant placement, and was treated with explantation.
CASE DESCRIPTION
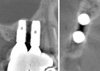
Case report protocol (KHD IRB 2010-1) was approved by the Institutional Review Board of Kyung Hee University Dental Hospital. A 67-year-old female was referred to the Department of Periodontology, Kyung Hee University School of Dentistry with chief complaints of pain on chewing and gingival swelling in the upper right molar area beginning 2 months previously. She was treated with non-surgical periodontal therapy and antibiotic administration for 1 month at a private clinic. Two dental implants had been placed with a ridge split in the upper right second premolar and the first molar areas at the private clinic 1 year earlier. The patient had taken medicine for hypertension and rheumatoid arthritis. She had been diagnosed with osteoporosis, and thus had a 1-year history of taking oral BPs, 70 mg alendronate (Fosamax, Merck, Whitehouse Station, USA) once per week. She had been taken off alendronate 5 months before her arrival at the Kyung Hee University School of Dentistry, because a bone density test and a Vitamin D test at the Department of Endocrinology showed a normal range. However, her serum C-terminal cross-linked telopeptide of type I collagen (CTX) level was low, measured at 21 pg/mL. On the first day of dental examination, she complained of pain on palpation, and gingival swelling and redness on the buccal side of the two implants. Exposure of the necrotic bone was observed between the upper right first premolar tooth and second premolar implant. However, we could not determine how long it had been exposed because the patient was reffered to us for treatment. The upper right second premolar implant showed 3 degrees of mobility, pain on percussion, and a 10-mm probing depth in the buccal and distal areas. Alveolar bone resorption with internal scattered residual bony fragments was seen between the two implants on a panoramic radiograph (Fig. 1) and computed tomography (Fig. 2). Widening of the periodontal ligament space and a radiolucent lesion in the apical area of the upper right first premolar were also seen.
During the first visit, inflammatory tissue around the implants was removed following flap reflection under local anesthesia, and the flap was sutured. Gingival swelling decreased after 1 week, but there was no change in exposure of the necrotic bone (Fig. 3). Explantation and extraction of the upper right first premolar was planned to prevent additional bone destruction. After an intrasulcular incision was made around the implants and the tooth to be extracted under local anesthesia, a vertical incision was done at the mesiobuccal line angle of the upper right canine. The full thickness flap was then elevated, and exposure of the implant threads was noticed on the buccal and inter-implant area (Fig. 4).
After extraction of the upper right first premolar, perforation on the buccal side of the extraction socket was seen and the extraction socket was also penetrated to the upper right second premolar implant distally at the apical area (Fig. 5). The two implants were removed with dental forceps and an elevator. The remaining granulated tissue was removed and a generalized ostectomy was done. The sharp edges of necrotic bone were trimmed by a high speed drill to prevent inflammation of the soft tissue and to manage pain. The remaining necrotic bone was partially (not entirely) removed by the high speed drill. Interestingly, during this procedure, distinct bone surface bleeding was not seen to any great extent (Fig. 6).
Tetracycline (50 mg/mL) irrigation was performed, and the flap was extended coronally to effect primary closure and was then sutured (Fig. 7). Amoxicillin 500 mg (Amoxapen®, Chong Kun Dang Pharmaceutical Co., Seoul, Korea) and Ibuprofen 200 mg (Brufen®, Sam-il Co., Seoul, Korea) were each administered for 1 week, and a mouth rinse with 0.12% chlorhexidine was recommended for the following 2 weeks. The following day, the patient complained of a slight fever, but it was relieved 2 days later. Stitch-out was done after 1 week (Fig. 8) and wound dehiscence was seen on the extraction socket of the upper right first premolar. The patient was instructed to keep using chlorhexidine as a mouth rinse. After 4 weeks, pin-point bone exposure was detected on the distal side of the upper right canine, but the patient did not have any discomfort or pain. After 4 months, no additional bone exposure was found at the operation site (Fig. 9), and there were no significant findings on the panoramic radiograph (Fig. 10). The patient is wearing a removable partial denture at the moment and receives follow-up care on a regular basis.
DISCUSSION
The patient in this case had a history of taking BPs for 1 year and no history of radiation therapy to the jaws, but there was no way to ascertain how long the necrotic bone had been exposed in the oral cavity because she was referred without any further information. However, we estimated that this patient met the three requirements of BRONJ as suggested by AAOMS [4] and thus was diagnosed with BRONJ.
Although there has not been sufficient research to determine the nature of BRONJ, some risk factors have been connected with an increasing tendency toward the incidence of BRONJ for patients taking BPs. Although few reports have investigated risk factors, it has been suggested that risk factors such as potency of BPs, period of taking BPs, and systemic/local factors could influence the incidence of BRONJ [6]. The more powerful potency of BPs and the longer period of taking BPs, the greater the occurrence of BRONJ. Local risk factors which increase the incidence of BRONJ are as follows: extraction, implant placement, surgical procedures including osteotomy, and anatomic structures such as tori. Systemic risk factors include old age, diabetes mellitus, use of steroids, cancer therapy, and smoking. The most common risk factors in dentistry are intraoral surgery such as extraction and implant placement. It was reported that the incidence rate of BRONJ in patients taking BPs who had intraoral surgery was seven times higher than that of those who did not have surgery [7]. In this case, the patient took alendronate for only 1 year. However, we assumed that old age (67-year-old patient), extraction and implant placement worked as negative risk factors for BRONJ.
BPs were divided into two types depending on administration method - intravenous infusion and oral administration. Patients taking oral BPs manifested less bone exposure and mild symptoms compared to patients with IV BPs [8]. It has been reported that oral BPs had a lower risk since it took longer to develop bisphosphonate-induced osteonecrosis because of a slower accumulation rate in the bone [2]. However, there are many patients taking oral BPs for the treatment of osteoporosis, so it is very important to assess risks, especially when patients took BPs for a long period of time (longer than 3 years). Marx et al. [9] suggested using serum levels of morning fasting CTX to assess patients' risks of developing BRONJ by oral administration of BPs. CTX shows the healing potential of bone as a marker of bone turnover [10]. This telopeptide fragment is cleaved from the main crosslink chains of collagen by the osteoclast during bone resorption. Therefore, its serum level is proportional to the osteoclastic activity. The CTX value can be used as a marker for deciding the optimal timing of surgical intervention. Marx et al. [9] assessed 30 cases of BRONJ, and based on 17 out of 30 patients who were still receiving BPs at the beginning of the study, they classified risks of developing BRONJ into 3 classes depending on the CTX value. In this population, CTX values less than 100 pg/mL were classified into a high risk group, values from 100 to 150 pg/mL into a moderate risk group, and values higher than 150 pg/mL into a minimal risk group. The authors suggested that clinicians might consider implementing a "drug holiday" to achieve the desired (low risk) CTX level before initiating oral surgical procedures. The CTX value was 21 pg/mL in this case, which means the patient was in the high risk group. She had a history of delaying intraoral minor surgery for 1 to 2 months in the Department of Oral and Maxillofacial Surgery, Kyung Hee University School of Dentistry after being referred to the Department of Endocrine Medicine.
One of the most common clinical features associated with BRONJ is an exposure of necrotic bone. In the early stages, radiographic changes are not noticed, and patients do not have symptoms. However, patients may have severe pain if secondary infection or trauma on soft tissue above the sharp edges of the exposed bone occurred [11]. In this case, the patient complained of pain on chewing and gingival swelling on the upper right 2 implants which were placed 1 year earlier, and necrotic bone was observed around the implants. The patient was diagnosed as possessing stage 2 of BRONJ by the criteria of AAMOS [4], and stage 2 treatment strategy was carried out - selective removal of necrotic bone. Only the sharp necrotic bone which triggered soft tissue inflammation and pain was removed. Antibiotics and analgesics were administered for the control of pain and mouth rinse with 0.12% chlorhexidine was recommended. Pinpoint bone exposure was observed at the surgical site, but it was covered by soft tissue in 6 weeks, and healing was satisfactory. The treatment objectives for patients with an established diagnosis of BRONJ are to alleviate pain, eliminate inflammation in soft and hard tissue, and minimize the progression of bone necrosis [6]. Surgical debridement is an effective treatment for necrotic bone [12,13]. Removal of necrotic bone which constantly irritates soft tissue and recontouring of the bony shape are needed [14]. However, it is difficult to expose viable bleeding bone for the surgical margin since BPs affect the entire jaw bone and the necrotic bone margin is indefinite. Therefore, custom osteotomy is impossible, and it is recommended that loose segments of bony sequestrum be removed without exposing uninvolved bone [15]. Marx et al. [16] reported that attempts to accomplish debridement, cover the exposed bone with flaps, or bone-contouring procedures have mostly been counterproductive and have led to further exposed bone, worsening of symptoms, and a greater risk for a pathologic fracture of the jaw. Therefore, those procedures were to be limited only to cases where there was no response to nonsurgical management or continuation of symptoms. Since necrotic exposed bone itself is not painful, it is suggested that it retained for the preservation of jaw structure and normal function.
In terms of implant failure related to BPs, Jeffcoat [17] reported a 100% success rate for 102 implants with no clinical evidence of infection, pain or bone necrosis in patients receiving oral BPs for a mean duration of 3 years. Madrid and Sanz [18] reviewed 1 prospective and 3 retrospective studies and reported that there was no BRONJ after implant placement in 217 patients who took oral BPs for less than 5 years. They concluded that oral BP administration did not affect the short term success rate of an implant (1 to 4 years). Although the implant failure rate due to BRONJ is low for patients administered oral BPs, implant failure is possible for patients who took BPs for only 1 year. Thus, it is suggested that if implant placement were planned, informed consent should be provided relating to possible future implant failure and osteonecrosis of the jaw for patients taking oral BPs. Discontinuation of oral BPs can be considered from 3 months prior to surgery to 3 months after surgery if the patient's systemic condition allows it, in cases where the administration period of BPs was greater than 3 years [4]. A number of studies have recently reported that the incidence of BRONJ decreased after discontinuation of oral BPs therapy [19,20].
As the aging population grows, the number of patients with osteoporosis increases, thus the number of patients taking BPs for the treatment of osteoporosis is also on the rise. Therefore, further consideration of the long term stability of BPs is needed. As we have discussed above, serum CTX could be used as a systemic marker for assessment for the risk of BRONJ; thus further studies about serum CTX are needed. In addition, more detailed studies should be conducted to decide if modification of a treatment plan for implant placement and extraction (depending on the period of administration) is necessary for patients taking oral BPs.









 XML Download
XML Download