

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Healing of an extraction socket is characterized by internal changes that lead to the formation of bone within the socket and by external changes that lead to the loss of alveolar ridge width and height [1]. The healing process following tooth extraction apparently results in a more pronounced resorption on the buccal aspect than the lingual/palatal aspects of the ridge [2]. As a result, in the case of advanced periodontitis, the width of the alveolar ridge is reduced and severe alveolar bone resorption occurs. These healing processes result in various complications-lack of available alveolar bone for implant placement, an unfavorable crown-implant ratio, as well as aesthetic problems in the anterior area.
Socket preservation is a procedure in which graft material or a scaffold is placed in the socket of an extracted tooth at the time of extraction to preserve the alveolar ridge. Various types of materials are used for this purpose, such as autogenous bone, allograft bone, xenograft materials, and alloplast materials [3-7]. There is much controversy surrounding the need for and efficacy of socket preservation. Some researchers argue that socket preservation cannot prevent the resorption of extracted socket walls, and that the quality of newly formed bone cannot be guaranteed due to graft materials. Others agree on the necessity of socket preservation, which can maintain the shape of soft tissue and hard tissue and reduce the need for an additional augmentation procedure.
Researchers have reported various socket preservation techniques using different graft materials. The most popular technique consists of filling in the extraction socket with xenograft material, covering it with a resorbable membrane, and then achieving primary closure [7]. Currently, bovine bone graft material is the most commonly used. However, the possibility of bovine spongiform encephalopathy cannot be completely ruled out when using a bovine bone graft [8]. For this reason, deproteinized horse bone-derived mineral materials were developed in our laboratory.
The purpose of this experiment is to clinically and histologically evaluate the results of using horse-derived bone mineral for socket preservation.
MATERIALS AND METHODS
This was a prospective study with a clinical trial. The study comprised 4 patients who were scheduled for extraction as a consequence of severe chronic periodontitis or an apical lesion. The extraction was followed by socket preservation to prevent alveolar bone resorption. This study was approved by The Institutional Review Board of Seoul National University Dental Hospital (CDE09002). Written informed consent was obtained from all patients. Exclusion criteria were as follows: age less than 18 years, current pregnancy or breast-feeding, wearing orthodontic appliances, presence of any sign of acute inflammation, history of systemic diseases that contraindicate surgical procedures, and being a heavy smoker (≥ 1 pack/1 day).
Surgical procedures
Periapical radiographs were taken using a long cone paralleling technique before socket preservation. Following local anesthesia and extraction, crestal and intrasulcular incisions were made to expose alveolar bone. Buccal and palatal flaps were reflected and socket dimensions were measured. Clinical parameters included buccal-palatal width, mid-buccal crest height, and mid-palatal crest height. The reference point was the cemento-enamel junction of the adjacent tooth.
Extracted sockets were grafted with horse-derived bone mineral (OCS-H, NIBEC, Seoul, Korea) and covered by placing barrier membranes (Bio-Gide, Geistlich Pharma AG, Wolhusen, Switzerland) over the graft (Fig. 1). For primary closure, periosteums were incised and the buccal flap was coronally advanced and sutured in a tension-free state.
Postoperative systemic antibiotics were prescribed for 14 days and mechanical plaque control was avoided for 4 weeks. 0.1% chlorhexidine digluconate solution was used twice a day for plaque control. Patients were evaluated regarding whether the graft or membranes were exposed and whether there were adverse reactions or inflammation in the adjacent areas at 7 days, 3 months, and 6 months and, if necessary, supragingival dental plaque was removed.
Periapical radiography was taken 6 months after socket preservation (Fig. 2). For implant installation, the flaps were reflected and the measurements were repeated at the time of re-entry. The specimens were harvested using a trephine bur in the process of implant site development.
Histologic analysis
Trephine cores were fixed in 10% neutral buffered formalin solution, dehydrated through a series of ethanol solutions of increasing concentrations and embedded in embedding media (Technovit 7200, Exakt, Hamburg, Germany). The embedded specimens were mounted on acrylic glass slabs and cut through the vertical plane with a diamond saw. The sections were ground and prepared for histologic analysis using the staining kit (Multiple Stain Kit, Polysciences, Warrington, PA, USA).
Histologic examination was conducted using a light microscope (BH-2, Olympus Optical, Osaka, Japan). After microscopic examination, a photograph of each slide was taken using a digital camera and the resulting images were saved to a computer for histomorphometric analysis. Measurement of each tissue component was carried out using an automated image analysis system (Tomoro Scope Eye 3.6, Techsan, Seoul, Korea).
Statistical analysis
Ridge width, buccal crest height, and palatal crest height were used for comparisons and statistical analysis. Comparisons between baseline and 6 months were performed using the Wilcoxon signed rank test. The data were reported as mean ± SD with a significance level of P < 0.05. A statistical software program was used for data analysis (SPSS, SPSS Inc., Chicago, IL, USA).
RESULTS
The four patients who had undergone socket preservation using horse-derived bone mineral were analyzed. No patients dropped out. Neither side effect nor adverse reactions were reported. No membrane exposure was observed. The surgical sites healed uneventfully. At the time of re-entry, newly formed hard tissues were observed at the socket preservation sites. Collagen membranes were not found at the surgical sites.
Horizontal and vertical ridge changes
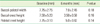
Changes in the horizontal and vertical ridge dimensions are shown in Table 1. The mean ridge width at baseline was 7.75 ± 2.75 mm, and at 6 months, 7.00 ± 2.45 mm. The ridge width exhibited no significant difference between baseline and 6 months. The mean buccal crest height at baseline was 7.5 ± 5.20 mm, and at 6 months, 3.50 ± 0.58 mm. The mean palatal crest height at baseline was 7.75 ± 3.10 mm, and at 6 months, 5.00 ± 0.82 mm. There were no significant differences in buccal and palatal crest heights between baseline and 6 months.
Histomorphometric analysis
Three specimens from the grafted sites were obtained for histologic evaluation. Histologic images showed new bone formation in contact with graft particles (Fig. 3). Results of the histomorphometric analysis are shown in Table 2. The amount of newly formed bone was 9.88 ± 2.90%, the amount of graft particles was 42.62 ± 6.57%, and the amount of soft tissue was 47.50 ± 9.28%. The graft particles were rarely resorbed by host immune cells.
DISCUSSION
The purpose of this experiment was to evaluate the efficacy of socket preservation using horse-derived bone mineral to prevent ridge collapse after tooth extraction. The results showed that socket preservation using horse-derived bone mineral can effectively maintain ridge dimensions following tooth extraction.
There are many studies about ridge dimensional changes following tooth extractions. Alveolar bones undergo wound healing processes after tooth extraction [9]. During these processes, the width and height of the alveolar ridge are drastically reduced, especially on the buccal bone side. Schropp et al. [1] reported that the width of the alveolar ridge was reduced 50%, and that two-thirds of the loss occurred in the first 3 months after extraction. Although various procedures such as immediate implant placement [10,11] and bone grafting [12] were attempted to prevent ridge resorption, no method has completely prevented physiological bone resorption. In particular, buccal bone is composed mostly of bundle bone, so it is vulnerable to this resorption [2,13]. A deficiency of available alveolar bone due to ridge resorption makes implant placement difficult and produces esthetic problems in the anterior sites. Based on these results, socket preservation is attempted in order to minimize ridge dimensional changes following tooth extraction. The maintenance of ridge dimensions following tooth extraction is important, particularly if implant placement needs to be delayed for several months.
Various socket preservation techniques have been introduced to maintain the hard and soft tissue dimensions of extracted sites. There are many kinds of graft materials for this purpose, such as demineralized freeze-dried bone allograft, autogenous bone, bioactive glass, hydroxyapatite, and deproteinized bovine bone mineral (DBBM) [3-7]. For barrier membranes, collagen membranes and e-PEFE have commonly been used. Several studies comparing grafted sockets with ungrafted sockets demonstrated that grafted sockets maintained significantly more ridge height and width dimension [14].
Among the many available methods of ridge preservation, the most commonly used method was DBBM graft covered by collagen membranes, followed by flap advancement to achieve primary closure. DBBMs are biocompatible, osteoconductive, and the appropriate graft material for the preservation of extraction sockets [15,16]. However, although DBBMs have been processed by deproteinization and heat treatment, the possibility of bovine spongiform encephalopathy cannot be completely ruled out. According to the previous report, the possibility of disease transmission is once per 1.3 × 1019 based on the methods of the German Ministry of Health [8]. Therefore, research for the development of alternative donor sources is necessary.
In this study, deproteinized horse-derived bone graft material was evaluated to determine its efficacy for socket preservation. Horse-derived bone mineral is made from natural hydroxyapatite derived from horse bone. Organic materials were effectively removed and no immune reactions were observed. It has porous structures, osteoconductivity and biocompatibility, so it can facilitate new bone formation when applied in bony defects. In comparisons of the clinical parameters between baseline and 6 months, ridge width, buccal crest height, and palatal crest height data showed no statistically significant changes. These results suggest socket preservation using horse-derived bone mineral can effectively maintain ridge dimensions following tooth extraction. Because graft materials are mainly confined to the intra-alveolar socket, ridge augmentation effects by graft materials could rarely be observed. The histomorphometric analysis exhibited 9.88% of newly formed bone. This result is inconsistent with previous studies evaluating the newly formed bone percentage after the placement of xenograft materials. This may be ascribed to a discrepancy in the evaluation criteria for histomorphometric analysis [15,17,18]. However, graft particles were well incorporated.
In conclusion, socket preservation using horse-derived bone mineral can effectively maintain ridge dimensions following tooth extraction and can promote new bone formation by means of osteoconductivity.




 XML Download
XML Download