

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endometrial cancer is the most common gynecological malignancy in Western countries [1]. Hysterectomy and bilateral salpingo-oophorectomy have been accepted as standard definitive surgical procedures. The role of lymphadenectomy in treating endometrial cancer is controversial because the therapeutic effect depends on variable factors [1234]. Lymphadenectomy is not useful in women with well differentiated tumors and superficial myometrial invasion because of the low incidence of lymph node metastasis [56]. However, the incidence of lymph node metastasis is markedly increased in women with poorly differentiated tumors and deep myometrial invasion [6].
Magnetic resonance imaging (MRI) is reported to be useful for estimating the tumor volume of endometrial or cervical cancer [78]. The volume index is compatible with myometrial invasion as a factor for predicting lymph node metastasis [7]. Lymph node metastasis is detected only in 1.1% of women with MRI-invisible cervical cancer following biopsy [8]. However, the treatment and prognosis of endometrial cancer that is not seen on MRI remain unclear. We hypothesized that the long-term outcomes of patients with MRI-invisible endometrial cancer is different from those in patients with MRI-visible endometrial cancer. The purpose of this study was to retrospectively evaluate the long-term outcomes of MRI-invisible endometrial cancer.
MATERIALS AND METHODS
This retrospective study was approved our Institutional Review Board (2015-07-084-002) and informed consent was waived.
1. Patients
Between February 1995 and December 2011, we identified a total of 721 patients for whom MRI was performed to evaluate endometrial cancer from our database (Fig. 1). Of these patients, we included 433 patients (median, 51 years; range, 22 to 82 years; interquartile range, 45 to 56 years) with endometrial cancer exhibiting invasion to less than half of the myometrium, no cervical extension, or no extra-uterine disease on MRI. A total of 288 patients were excluded for the following reasons: MRI-staged IB or higher endometrial cancer (n=228), loss to follow-up (n=41), no MRI examination (n=17), and no surgery (n=2).

MRI-staged IA endometrial cancers were divided into MRI-invisible and MRI-visible cancers. Of 433 patients, 89 (median, 49 years; range, 22 to 72 years; interquartile range, 43 to 54 years) had MRI-invisible cancer and 344 (median, 52 years; range, 21 to 82 years; interquartile, 46 to 56 years) had MRI-visible cancer (Table 1). Both cancers were treated via simple hysterectomy with (n=393) or without (n=40) lymph node dissection. The indications for pelvic or para-aortic lymphadenectomy depended on the surgeon's decision.
Table 1
Patients' demographics of MRI-staged IA endometrial cancers

Values are presented as median (range) [25%–75% interquartile range] or number (%). When a residual tumor was not found in the postoperative pathologic specimens, the diagnoses of preoperative cytology or biopsy were used. Mann-Whitney test was used to compare two groups regarding age, body mass index, CA-125 levels, and the follow-up period. Fisher's exact test was used to compare two groups regarding cell type.
MRI, magnetic resonance imaging; BMI, body mass index; Endo, endometrioid adenocarcinoma; CA-125, cancer antigen 125.
2. MRI examination
MRI was performed after endometrial cancer was histologically proven via endometrial biopsy. This examination was conducted using a 1.5T MR scanner (Signa, GE Medical System, Milwaukee, WI, USA) or a 3.0T MR scanner (Intera Achiva 3T, Philips Medical System, Best, The Netherlands). MRI-invisible cancer was diagnosed when the lesion was not visible on T2-weighted images, T1-weighted images, and post-contrast images (Fig. 2). MRI-visible cancer was diagnosed when the lesion was hypointense on T2-weighted images, and was enhanced on post-contrast MR images compared to T1-weighted images (Fig. 3). Endometrial hematoma was defined when the lesion was hypointense on T2-weighted images, hyperintense on T1-weighted images, but was not enhanced on post-contrast MR images.
Fig. 2
Magnetic resonance imaging (MRI)-invisible 1A endometrial cancer in a 68-year-old woman. A T2-weighted sagittal image shows no focal lesion within the hyperintense endometrium (arrows). Prior to the MRI scan, endometrial biopsy revealed grade II endometrioid adenocarcinoma. Pathologic examination following hysterectomy confirmed no residual cancer but scattered atypical endometrial glands. There was no metastasis in the pelvic and para-aortic lymph nodes. No recurrent cancer has been found for postoperative 49 months.
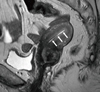
Fig. 3
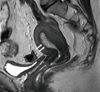
Magnetic resonance imaging (MRI)-visible 1A endometrial cancer in a 47-year-old woman. A T2-weighted sagittal image shows an endometrial cancer invading the superficial myometrium (arrows). Pathologic examination following hysterectomy confirmed a 4.3 cm grade I endometrioid adenocarcinoma invading superficial myometrium. There was no metastasis in the pelvic lymph nodes. No recurrent cancer has been found 46 months after surgery.
3. Data analysis
MR images were reviewed by two readers. One was a radiologist who had 16 years of experience and the other was a fourth-grade resident in the Department of Radiology. They reached a diagnosis in consensus. When MR images were reviewed, the readers were given only “endometrial cancer” and other clinicopathologic information was not disclosed.
MRI-invisible and MRI-visible cancers were compared regarding patient age, cancer antigen 125 (CA-125) levels, and histologic diagnoses. The International Federation of Obstetrics and Gynecology (FIGO) stages of these groups were recorded for comparisons. The postoperative histologic findings of MRI-invisible and MRI-visible cancers were described and compared regarding the tumor size, depth of myometrial invasion, lymph node metastasis, and other extra-uterine metastases that were not identified on MRI. The lesion sizes and depth of invasion were measured using hysterectomy specimens.
MRI-invisible and MRI-visible cancers were compared regarding the local or distant recurrent rate, recurrence-free survival rate, and overall survival rate. The organs affected by distant metastasis in patients with MRI-invisible and MRI-visible cancers were recorded for comparisons.
4. Statistical analysis
Fisher's exact text was used to compare MRI-invisible and MRI-visible cancers regarding residual tumor, histologic diagnoses, cancer grade, myometrial invasion, lymph node metastasis, and recurrence rates.
Mann-Whitney test was used to compare MRI-invisible and MRI-visible cancers regarding patient age, body mass index, CA-125 level, lesion size, and the follow-up period.
Multivariate regression model was used to evaluate the correlation of MRI finding and myometrial invasion and lymph node metastasis. Firth's penalized maximum likelihood estimation method due to rare events was in logistic regression model. Recurrence-free and overall survival rates were compared between MRI-invisible and MRI-visible cancers using a Cox regression model.
SAS ver. 9.4 (SAS Institute, Cary, NC, USA) and R 3.0.3 (Vienna, Austria; http://www.R-project.org/) and IBM SPSS ver. 23 (IBM Co., Armonk, NY, USA) were used for statistical analysis. A two-sided p<0.05 was considered statistically significant.
RESULTS
A total of 10 cases were discordant between a staff radiologist and a resident. These cases were reviewed together, and were reached to final diagnoses in consensus. We did not evaluate these discordant cases regarding histologic data and outcomes because the number was too small.
Women with MRI-invisible cancer were younger than those with MRI-visible cancer (p=0.012) (Table 1). The median sizes of MRI-invisible and MRI-visible cancers were 4 mm (range, 0 to 40 mm; interquartile range, 0 to 13 mm) and 20 mm (range, 0 to 88 mm; interquartile range, 12 to 33 mm), respectively (p<0.001). Residual tumors were not detected in 55% (49/89) of patients with MRI-invisible cancer and in 7% (25/344) of patients with MRI-visible cancer (p<0.001). The follow-up period of all MRI-staged IA endometrial cancers ranged from 8 to 240 months (median, 94 months; interquartile range, 71 to 133 months). The median follow-up period of patients with MRI-invisible cancer was longer than that for patients with MRI-visible cancer (p=0.013). However, there was no difference between the MRI-invisible and MRI-visible cancer groups in terms of body mass index (p=0.518), preoperative CA-125 levels (p=0.183), and the ratio of endometrioid adenocarcinoma to non-endometrioid cancer (p=0.343).
The FIGO stages of MRI-invisible cancer were IA in 86 (96.6%) and IB in 3 (3.4%), while those of MRI-visible cancer were IA in 332 (96.5%), IB in 1 (0.3%), IIIC1 in 9 (2.36%) and IIIC2 in 2 (0.6%). No MRI-invisible cancers had a FIGO stage II or higher. Myometrial invasion was histologically detected in 20.2% (18/89) of patients with MRI-invisible cancer and in 56.7% (195/344) of patients with MRI-visible cancer (p<0.001) (Table 2). Invasion to less than half of the myometrium was seen in 16.9% (15/89) of patients with MRI-invisible cancer and in 56.4% (194/344) of patients with MRI-visible cancer. Invasion to more than half of the myometrium was seen in 3.4% (3/89) of patients with MRI-invisible cancer and in 0.3% (1/344) of patients with MRI-visible cancer. The incidence of myometrial invasion was also significantly different between the two cancer groups after adjustment for tumor size.
Table 2
Pathologic parameters of MRI-staged IA endometrial cancers

Values are presented as median (range) [25%–75% interquartile range] or number (%). When cancer cells were not found in the postoperative pathologic examination, they were excluded from this table. Mann-Whitney test was used to compare two groups regarding lesion size. Fisher's exact test was used to compare two groups regarding histologic diagnoses, myometrial invasion and lymph node metastasis.
MRI, magnetic resonance imaging; Endo, endometrioid adenocarcinoma.
*Includes mucinous adenocarcinoma, squamous cell carcinoma, sarcoma, small round cell tumor, poorly differentiated.
Only one patient with MRI-invisible cancer had multiple recurrent tumors in the vault and peritoneum. Twenty-seven patients with MRI-visible cancer had multiple local or distant recurrent tumors. Distant metastases were observed in 11 patients with MRI-visible cancer. Organs affected by distant metastasis other than lymph node in patients with MRI-visible cancer were lung (2.3%, 8/344), liver (0.87%, 3/344), and others (0.3%, 2/344). Two patients showed multi-organ distant metastasis. One patient had metastases to the liver and brain, and the other had metastases to the lung and liver.
Lymph node metastases on pathologic examination were detected in 0% (0/86) of patients with MRI-invisible cancer and in 3.2% (11/344) of patients with MRI-visible cancer. During the follow-up period, recurrent tumors in lymph nodes were detected in 0% (0/86) of patients with MRI-invisible cancer and in 1.4% (5/344) of patients with MRI-visible cancer. Metastasis or recurrence in lymph nodes was not detected in patients with MRI-invisible cancer, compared to 4.7% (16/344) of patients with MRI-visible cancer (p=0.052). However, the incidence of metastasis or recurrence in lymph nodes was significantly different between the two cancer groups after adjustment for tumor size (p=0.027).
On pathologic specimens, MRI-visible cancer metastasized to pelvic lymph node in 3.0% (9/304) of the 304 patients undergoing pelvic lymphadenectomy and to para-aortic lymph node in 1.8% (2/113) of the 113 patients undergoing para-aortic lymphadenectomy. On follow-up imaging studies, MRI-visible cancer metastasized to pelvic lymph node in 0.3% (1/344), to para-aortic lymph node in 0.3% (1/344), or to other lymph node in 0.87% (3/344).
The recurrence rates of MRI-invisible and MRI-visible cancers were 1.1% (1/89) and 7.8% (27/344), respectively (p=0.026). The recurrence-free rates of these cancer groups were 98.9% (88/89) and 91.6% (315/344) (p=0.022) (Fig. 4), respectively. The overall survival rates of the two cancer groups were 97.8% (87/89) and 93.3% (321/344), respectively (p=0.087).
Fig. 4
Recurrence-free survival rates of magnetic resonance imaging (MRI)-invisible and visible endometrial cancers. The graph illustrates that patients (blue) with MRI-invisible endometrial cancer have a higher recurrence-free survival rate than patients (green) with MRI-visible endometrial (p=0.022). The survival rates of these cancer groups are 98.9% (88/89) and 91.6% (315/344), respectively.

DISCUSSION
MRI has been accepted as a reliable tool for measuring the size or volume of endometrial [79101112] or cervical [8131415] cancer prior to hysterectomy. As tumor size or volume measured with MRI decreases, cancer stage becomes lower. Subsequently, lymph node metastasis becomes less likely. From this point of view, if MRI does not depict any residual tumor in patients with endometrial cancer following biopsy, this can indicate that the tumor burden is lower than that of MRI-visible endometrial cancer. Park et al. [8] reported that lymph node metastasis occurs only in 1.1% of patients with MRI-invisible IB1 cervical cancer.
Myometrial invasion is one of the independent factors predicting lymph node metastasis [5]. When deep (≥50%) myometrial invasion is present, lymph node metastasis is detected in more than 30% of the patients. However, when superficial (<50%) myometrial invasion is present, lymph node metastasis occurs only in 5% of the patients [16]. A meta-analysis of prospective studies reported the utility of MRI in preoperatively estimating the depth of myometrial invasion [17]. However, interobserver agreement was variable in assessing myometrial invasion with MRI. Multi-center studies showed that the sensitivity of MRI for detecting deep myometrial invasion decreases to 54% while that for endometrium-confined cancer or superficial myometrial invasion increases to 89% [18]. Tanaka et al. [19] shows that the use of intraoperative frozen section is associated with a higher agreement rate than MRI in evaluating myometrial invasion. Nevertheless, they consider MRI to be an acceptable modality for determining a preoperative surgical plan regarding lymphadenectomy especially in grade 1 or 2 endometrioid adenocarcinoma [19].
Kang et al. [20] developed a preoperative risk prediction model for lymph node metastasis using preoperative CA-125 levels and MRI findings. They found that lymph node metastasis occurs in 1.3% of patients with endometrial cancer who meet the following criteria: endometrioid histology by endometrial biopsy; <50% myometrial invasion with no extension beyond the corpus and no enlarged lymph nodes according to MRI; and CA-125 levels ≤35 IU/mL before surgery. This model was reproducible in a Korea-Japan cooperative study showing that lymph node metastasis occurs in 1.9% of patients with low risk endometrial cancer [21]. They [22] also suggested that a good risk prediction model should provide a false-negative rate of <2% in predicting lymph node metastasis, assuming that the prevalence of lymph node metastasis is 10% using three previously reported models [62324].
Our study demonstrated that lymph node metastasis was not detected in patients with MRI-invisible endometrial cancer. The nodal metastatic rate of patients with MRI-invisible cancer appears to be lower than that of patients with low risk endometrial cancer, as reported in previous studies [16202122]. Lymph node metastasis becomes less likely as the size or volume of endometrial cancer as assessed via MRI decreases [47]. For this reason, lesion invisibility on MRI could be an extremely strong biomarker for predicting no lymph node metastasis. Todo et al. [7] reported that tumor size is more easily measurable on preoperative MRI. However, it is not easy to measure small, flat, poorly demarcated, or multiple lesions on MRI. Determining whether or not a lesion is visible on MRI appears to be easier for radiologists and gynecologists than measuring lesion size on MRI.
Our study also showed that cancer recurrence in lymph nodes was not detected on follow-up imaging examinations. Lesion invisibility on MRI appears to be a good prognostic factor for long-term outcomes among patients with endometrial cancer. Endometrial cancer may recur in lymph nodes during follow-up even if the lesion was considered a low-risk tumor. As a result, it is questionable whether lymph node dissection is necessary to improve the long-term outcomes of patients with MRI-invisible endometrial cancer.
Mariani et al. [24] have reported that patients who have FIGO grade 1 or 2 endometrioid corpus cancer with myometrial invasion ≤50% and without intraoperative evidence of macroscopic disease can be treated optimally with hysterectomy only, thereby avoiding the costs and morbidity associated with lymphadenectomy. Myometrial invasion and histologic grade are the most important prognostic indicators for early-stage endometrial cancer, and correlate well with the prevalence of lymph node metastases and patient survival. MRI is reserved for evaluating extrauterine disease as indicated by clinical symptoms, physical findings or abnormal laboratory findings. High risk endometrial cancers (e.g., serous, clear, carcinosarcomas, G3 endometrioid) are more aggressive histologic variants of malignant epithelial tumors, with a higher incidence of extrauterine disease at presentation.
However, we do not agree that MRI is reserved only for detecting extra-uterine metastasis from endometrial cancer. Todo et al. [7] have demonstrated that MRI can measure precisely the volume of endometrial cancer. Kang et al. [20] have addressed that MRI finding is one of criteria to determine whether or not pelvic lymph dissection is necessary. They have reported the incidence of lymph node metastasis was 1.9% in patients with low risk endometrial cancer using their criteria. Our study showed that MRI-invisible endometrial cancer was an excellent prognostic factor so that we were not able to find lymph node metastasis in the histologic examination in patients with MRI-invisible endometrial cancer. This is why this MRI finding is strongly suggesting a much lower tumor burden than MRI-visible IA endometrial cancer. Therefore, we think that MRI-invisible endometrial cancer appears a more important feature than myometrial invasion (<50%) and/or low-risk cancer in predicting lymph node metastasis. Furthermore, there was no difference between MRI-invisible and MRI-visible cancer groups in terms of histologic grades in our study. Indeed, we just wanted to reveal that MRI-invisible endometrial cancer may not require pelvic lymph node dissection regardless of histologic grades. Good MR image quality and meticulous interpretation are essential to identify MRI-invisible endometrial cancer.
Our study has some limitations. First, our study was conducted in a retrospective manner. Thus, selection bias cannot be completely excluded. Second, endometrial cancer was only evaluated using T2-weighted imaging, T1-weighted imaging, and contrast-enhanced imaging, as newer MRI techniques were not available for assessing endometrial cancer during the study period. Third, 1.5T and 3.0T MRI were both used for analysis. 3.0T MRI provides faster imaging acquisition and higher resolution imaging than 1.5T. There could be differences between these two imaging modalities regarding image quality. Fourth, interobserver agreement was not performed. MR images were reviewed in consensus by two readers who had different levels of experience in imaging interpretation. Fifth, MRI was not a mandatory examination for the preoperative evaluation of endometrial cancer. Lastly, the cost and effectiveness of MRI concerning the treatment of endometrial cancer were not assessed.
In conclusion, MRI-invisible endometrial cancer can be treated less invasively than MRI-visible endometrial cancer because of its lower tumor burden and better prognosis. Furthermore, lymphadenectomy and follow-up imaging in this cancer group do not show lymph node metastasis or recurrent cancer in lymph nodes. Therefore, lymph node dissection can be omitted if endometrial cancer is not visible on preoperative MRI.
 XML Download
XML Download