

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The effects of estrogen and progesterone are mediated by specific transmembrane receptors. Estrogen receptor (ER) and progesterone receptor (PR) are well-known prognostic factors in endocrine organ cancers. The clinical relevance of these receptors has been clearly established for endometrial and breast cancers [1]. There is currently a wide range of theories about ovarian carcinogenesis. However, recent evidence suggests that steroid hormonal stimulation may be implicated in the development and prognosis of ovarian malignancies. Thus, the study of steroid receptors in the ovary takes on an added importance [2,3].
Estrogens are main regulators of growth and differentiation in ovarian cells. Recent laboratory and preclinical data suggest that estrogens may exert a mutagenic effect on normal epithelial ovarian cells. In contrast, progesterone may offer protection against the mutagenic effects of estrogens by blocking cell growth and inducing cell differentiation and apoptosis. Studies addressing the potential carcinogenic or anticarcinogenic effects of these steroids generally examine mRNA transcription and ER/PR protein expression [4,5]. However, multiple technical dissimilarities between studies, in addition to the small samples evaluated in many reports precluded any conclusive analysis of the role of steroid receptors in the ovary.
Some authors have advocated that ER and/or PR expression may predict the survival of women with ovarian carcinomas [1-3,6-16], whereas several other reports have failed to detect such an association [17-19]. Attempts to define typical steroid receptor profiles among ovarian histologic types have been made. Reasons for failure in these attempts and for the different results obtained in previous studies can be attributed to the dissimilar techniques used to analyze steroid receptor expression and a low level of agreement between histologic evaluations.
Inconclusive data from previously published studies on ovarian cancer prognosis in relation to steroid hormone expression, prompted us to investigate the large dataset of ovarian carcinomas with a long-term follow-up period in our service. We evaluated the patterns of ER/PR expression between different histologic types of epithelial ovarian neoplasms, borderline ovarian tumors (BOTs) and carcinomas. The disease-free survival (DFS) and overall survival (OS) of women diagnosed with carcinomas in relation to steroid receptor expression were also studied.
MATERIALS AND METHODS
1. Patient selection
For this retrospective cohort study, we selected women undergoing surgical treatment for BOTs or ovarian carcinoma from 1993 to 2008 at the State University of Campinas-UNICAMP, São Paulo, Brazil. All study participants had surgeries classified as surgical staging (disease restricted to the ovaries) or cytoreductive surgery (advanced disease). The sample included women undergoing complete or incomplete staging and optimal or suboptimal cytoreduction. Follow-up data were retrieved up until December 2010. Excluded from the study were all women 1) undergoing neoadjuvant chemotherapy, 2) whose paraffin blocks were unavailable or inadequate, and 3) with other synchronous or metastatic tumors to the ovary. We assessed pathological and clinical (including follow-up) data from 38 BOTs and 172 ovarian carcinomas cases, totaling 210 women. Clinical data were collected from patient medical records. Patient age, menopausal status, tumor histologic type and grade, disease stage [20], and surgical outcomes (optimal or suboptimal surgery) were recorded.
In our institution, surgical staging of BOT included peritoneal washings, total abdominal hysterectomy, bilateral salpingo-oophorectomy with omentectomy, as well as pelvic and abdominal peritoneal biopsies. In selected patients, who desired childbearing and had BOT or stage I carcinomas (restricted to the ovary), unilateral salpingo-oophorectomy (fertility-sparing surgery) was performed. For ovarian carcinoma, surgical staging included peritoneal washings, total abdominal hysterectomy, bilateral salpingo-oophorectomy, omentectomy, pelvic and paraaortic lymph node biopsies with pelvic and abdominal peritoneal biopsies. Cytologic examination of ascitic fluid or peritoneal washings was performed in all cases. For advanced disease in BOTs or ovarian carcinomas, surgery included total abdominal hysterectomy, bilateral salpingo-oophorectomy with omentectomy and debulking to remove as much of gross tumor as possible. Cytoreduction was deemed "optimal" when residual implants measuring less than 1 cm were left. The presence of ascites was evaluated either by ultrasound or computed tomography (CT) scan or intraoperative examination. Histologic classification of ovarian tumors was performed, following World Health Organization (WHO) and International Federation of Gynecology and Obstetrics (FIGO) recommendations [20,21]. Patients underwent chemotherapy regimens with carboplatin, receiving either paclitaxel or cyclophosphamide, according to service protocol.
This study was approved by the Research Ethics Committee of the State University of Campinas (protocol number 1086/2009).
2. Specimens
Samples for tissue microarray (TMA) were obtained from the original paraffin blocks. All hematoxylin and eosin (H&E) stained slides were reviewed by an experienced pathologist to select the paraffin blocks most suitable for TMA sampling, i.e., those having unequivocal areas of BOT or ovarian carcinoma. Two areas of interest corresponding to the most representative areas of the tumor were marked and selected from each case for TMA construction. These marks guided the 1.0 mm cylindrical core of the paraffin blocks, which was performed using a TMA instrument (Beecher Instruments Microarray Technology, Silver Springs, CA, USA). TMA processing and analysis were performed, according to standard protocols that have been fully validated in ovarian pathology [22].
3. Assay methods
Immunohistochemistry (IHC): Four-micrometer TMA sections were deparaffinized with xylene and dehydrated in graded alcohols, according to normal protocols. For antigen retrieval, a commercially available pressure cooker (Pascal, Dako, Carpenteria, CA, USA) was used, immersing the slides in citrate buffer solution, pH 6.0 for 30 minutes. The slides were allowed to air-dry at room temperature and then washed in distilled water. The sections were incubated in a humid chamber with the specific primary antibodies at 4℃ overnight. We assessed the ER α subtype (ER, clone 1D5; Dako) [2,4]. Only the PR-A subtype is appropriate for IHC detection (PR, clone PgR 636; Dako) [2,23]. Internal and external, positive and negative controls were used to validate the reactions. Subsequently, the slides were washed in phosphate buffered saline [PBS], pH 7.4, incubated in ADVANCE HRP Detection System (Dako) at 37℃ for 1 hour, and washed in PBS. DAB chromogen substrate (3-diaminobenzidine, Sigma-Aldrich, St. Louis, MO, USA) was applied, at a proportion of 0.06 g to 100 mL of PBS, 500 µL hydrogen 3% peroxide and 1 mL dimethyl sulfoxide at 37℃ for 5 minutes. The slides were washed with water and counterstained with Harris' haematoxylin for 30 to 60 seconds, dehydrated, cleared and mounted on Entellan resin (Merck, Darmstadt, Germany). Internal and external, positive and negative controls were used for validation of the reactions [22].
4. Evaluation and interpretation of IHC
A single pathologist, who was blinded to the clinical and pathological data, scored the samples. Two TMA cores from each tumor were used for each marker, i.e., each tumor was assessed twice. If scores differed in both areas, the stronger staining was considered. Nuclear staining of ER and PR were recorded, as follows: 0, negative; 1, less than 1% stained nuclei; 2, 1% to 10% stained nuclei; 3, 10% to 35% stained nuclei; 4, 35% to 75% stained nuclei; 5, ≥75% stained nuclei. Nuclear staining intensity was also categorized as: 1, weak; 2, moderate;
3, strong. The final score was the sum of the percentage score of stained nuclei (ranging from 0-5) plus intensity score of the reaction (1-3). Therefore, the possible final scores were 0 (no staining), 2 (less than 1% and weak), 3, 4, 5, 6, 7, and 8. For statistical purposes, the final IHC ER/PR status was considered positive, when the score was ≥4 (Fig. 1).
5. Statistical analysis
Statistical analyses were performed by using the R Environment [24] statistical software package, with 95% confidence intervals (CI). Chi-square tests (and Fisher's exact tests, when required) were used to compare the clinical characteristics of women with BOT or ovarian carcinoma, and to evaluate steroid hormone expression among the histologic samples. A multivariate generalized linear model using binomial distribution (logistic regression) was fit to evaluate the combined ER/PR status of ovarian carcinomas, related to clinical and pathological features. We obtained a median follow-up period of 42 months (range, 17 to 60 months; 50% central-range). Sample size calculations for the survival models resulted in a sample requiring 105 subjects with complete follow-up. We used the multivariate Cox proportional hazards analysis to calculate the hazard ratios (HR) of DFS and OS which were defined as times elapsed since the main surgical procedure to time of disease recurrence and death from ovarian cancer, respectively, in relation to clinical and pathological characteristics. There was no significant event (relapses or deaths) in women with BOTs. The Kaplan-Meyer representation was used to assess OS in relation to patterns of ER/PR expression stratified by disease stage (stage I vs. stages II-IV). The curves were then compared using the Mantel-Cox log-rank method.
RESULTS
The mean patient age was 41.3 years (standard deviation [SD], 13.7) for BOT, and 54.7 years (SD, 12.6) for ovarian carcinomas (p<0.01). The BOT group consisted of 26.3% serous and 73.7% mucinous tumors. The histologic type of most ovarian carcinomas (46%) was serous type, followed by mucinous type (25%). Approximately 10% were mixed or endometrioid types. The majority (58%) of ovarian carcinomas were diagnosed at an advanced stage (6% were already stage IV). Disease recurrence was detected in 4 (27%) women with stage I serous carcinomas and in 39 (59%) women with stage II-IV disease. The primary surgical procedure was considered suboptimal for 66 (38%) women with ovarian carcinomas. Platinum-based chemotherapy drugs was for 133 (76%) women (data not shown). Most BOT and carcinomas were ER and/or PR negative, while 65.8% of BOT and 52.3% of carcinomas were negative for both receptors. There was no significant difference in steroid receptor expression, when BOT was compared to ovarian carcinoma (p=0.55 for ER alone, 0.90 for PR alone and 0.12 for combined expression) (Table 1).
In BOT, ER and PR expression (alone or combined), was significantly higher in serous than in mucinous tumors (p<0.01). In carcinomas, ER expression was significantly higher in serous vs. mucinous (p<0.01) and clear cell tumors (p<0.01), and in endometrioid vs. mucinous type (p<0.01). PR expression was significantly higher in serous vs. mucinous (p<0.01) and in endometroid vs. mucinous (p<0.01) and vs. serous (p=0.03). Considering both receptors, the level of expression was significantly higher in serous vs. mucinous (p<0.01) and clear cell (p=0.02) tumors. Other pairwise comparisons were non-significant. Overall, endometrioid ovarian cancer showed the highest (82.4%) ER and/or PR expression among all types of ovarian cancer, whereas mucinous ovarian cancer showed the lowest (13.6%) ER and/or PR expression (Table 2).
Steroid receptor expression in ovarian carcinomas revealed no significant stage-related difference. The vast majority (>80%) of endometrioid tumors were positive for at least one steroid receptor, regardless of tumor stage. Seven (100%) stage I clear cell carcinomas were negative for both receptors. Of the 3 cases of stage II-IV clear cell tumors, two were positive for at least one receptor (data not shown). In Tables 3 and 4, tumors with similar patterns of ER/PR expression were grouped together (mucinous, clear cell and others vs. serous and endometrioid). In general, serous and endometrioid tumors were predominantly ER/PR positive, whereas mucinous and clear cell tumors were preponderantly ER/PR negative (OR, 4.61; 95% CI, 2.07 to 10.25; p<0.01). Other tumor characteristics were not significantly associated with ER/PR status.
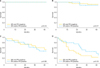
Neither the epidemiological and clinical features studied, nor combined steroid receptor status affected DFS (Table 4). The probability of death was found to be significantly higher (HR, 4.0; 95% CI, 1.6 to 10.3; p<0.01) in women with advanced disease (stages II-IV), and for those with residual disease after surgery (suboptimal surgery) (HR, 2.12; 95% CI, 1.15 to 3.9; p<0.01). Survival curves for women with ER and PR negative tumors versus ER and/or PR positive tumors, stratified by disease stage and tumor type, revealed no significant difference in survival (Fig. 2).
DISCUSSION
In our study, there was no difference in ER or PR expression between BOT and ovarian carcinoma. However, we detected a significant difference in ER/PR expression among the histologic types of carcinomas. Most serous and endometrioid carcinomas were ER positive, leading us to group them together in subsequent analyses. Conversely, mucinous and clear-cell carcinomas were ER and PR negative tumors in general. The same tendencies were observed in BOT, although we recognize that the size of our BOT sample was very limited. ER and PR expressions, alone or combined, were not related to either DFS or OS in women with ovarian carcinoma.
The clinical significance of steroid receptor status for the prognosis of ovarian cancer is still unclear. In theory, since estrogen affects the development of the ovarian follicles and ovarian cancer cell lines, dependent on ER expression, ER status should be associated with a difference in survival. On the other hand, progesterone inhibits DNA synthesis and cell division, and thus it may exert a protective prognostic effect on women with ovarian cancer [25]. Several reports have shown no significant difference in survival with increasing levels of PR expression [17-19] , while few reports have indicated that a higher ER status correlates with increased survival [7,11]. Other authors have reported that a higher PR status is associated with increased survival [1-3,5,8-10,12-14,16]. However, significant methodological dissimilarities exist between studies, and discrepancies in the reports may be attributed to these methodological issues. For instance, earlier works were performed using the dextran-coated charcoal (DCC) method [7,9,11-14,16-19]. The DCC method produced false-positive results if the surrounding benign tissue expressed the receptor on stromal cells [2]. IHC is currently the standard for ER/PR detection, allowing for precise detection of the receptors in tissues of interest [2,22].
Our findings are in agreement with results from previous reports on ER/PR expression in different histologic types of epithelial ovarian tumors [2-5]. Taken together, previous findings indicate that serous and endometrioid tumors express ER and/or PR. Endometrioid tumors have been reported to primarily express PR, whereas mucinous tumors are most likely to be ER and PR negative [2-5]. Restricting our literature search to IHC-based studies, we found that frequencies of ER and PR expression varied from 38% to 77% (mean, 59%) and from 26% to 43% (mean, 33%), respectively [1-3,5,8-10]. Using IHC, we found a somewhat lower prevalence of ER (35.5%) and PR (27%) positive ovarian carcinomas in our series.
A few studies have suggested that PR positive status is an independent prognostic factor, associated with better survival in multivariate analysis [3,5,8,10]. Other studies failed to demonstrate or only indicated a trend towards a correlation between PR status and a favorable survival. However, this was not shown to be significant, either by univariate or multivariate analysis [11]. It is worth mentioning that DCC-based studies [17-19] also found no relationship between DFS and OS and ER/PR status in ovarian carcinomas. Other important aspects were examined in those studies, e.g., the relationship between steroid receptor status and response to chemotherapy [19], surgical stage [17,19] and histologic type and grade [19], but all those analyses yielded negative results.
In a study of 106 cases [2], ER positive expression did not show any association with DFS or OS, whereas PR positive expression had a significantly positive influence on survival in univariate analysis. Both median DFS and OS in patients with tumors expressing PR positive were significantly longer than those in patients with PR-negative tumors. Of the 4 alternative combinations of ER positive/negative and PR positive/negative expressions, the best prognostic indicator of DFS and OS was found in patients with ER-/PR+ expression, compared to women with tumors showing any of the other 3 combinations. However, there were no statistically significant differences. The effects of PR status disappeared on multivariate analyses, and the remaining factors associated with survival were disease stage and response to first-line chemotherapy. A recent report [10] detected that ER alone, in contrast to PR alone, had no prognostic value. However, those authors investigated combined ER/PR expression and found that ER-/PR+ tumors were particularly associated with an increased overall survival, compared to PR+ tumors. Using IHC, Munstedt et al. [10] found a positive influence of ER-/PR+ tumors on patient survival in both uni- and multivariate analyses. In addition, PR was inversely correlated with tumor stage and high degree of differentiation, findings that were in accordance with another study [8].
Although Lee et al. [8] failed to demonstrate any prognostic value of the ER receptor, patients with PR expression >10% were shown to survive longer than patients with <10% PR expression levels. In the Cox proportional hazards analysis, only disease stage and PR were significant among all the factors that influence survival. ER did not show any effect on survival. Furthermore, the combined expression of both markers showed no greater significance than PR alone. In a study by Kommoss et al. [9], ER has been shown to be of no significant prognostic value. Survival was significantly better in patients with PR positive tumors (IHC and DCC) in univariate analysis. According to that report, residual tumor after primary surgery was the only significant prognostic factor remaining after multivariate analysis. Contrary to all other IHC studies, the largest series to date [3] has detected more favorable outcomes for women with ER and/or PR positive carcinomas.
Our study does not support the positive influence of PR on prognosis, and corroborates previous findings indicating that ER is of no prognostic value. In our study, the only factors that have a significant association with survival after multivariate scrutiny are advanced tumor stage (II-IV) and residual disease after primary surgery. Both factors are well-known predictors of poor prognosis.
In agreement with results from previous reports, our study clearly suggests that there is a need for a thorough review of the role of steroid receptor status in ovarian cancer. No definitive assumption can be made on the value of investigating ER/PR expression in either ovarian carcinomas or BOT in clinical practice.





 XML Download
XML Download