

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
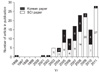
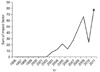
Although laparoscopic surgery was started in 1990 from cholecystectomy in Korea, there were long time gap to begin gastrectomy. Because D2 or D2 plus alpha gastrectomy had been accepted as a standard surgery at that time, laparoscopic surgery was just naïve looking for skillful gastric surgeons. Conservative surgeons never dreamed trying laparoscopic gastrectomy (LG) although they have acknowledged Kitano's paper for at least 15 years. Confronting conservative opinions, young courageous and ambitious surgeons tried various advanced procedures and also felt Instruments and energy device was not enough to guarantee delicate dissection for gastric cancer. However, gradual technological development follows surgeon's imagination and need for minimal invasive surgery (MIS). In the late 1990s, at least four surgeons began LG. In the year 1995, Kim(1) presented video for LG in the Korean Surgical Society (KSS) meeting for the first time, but there were strong critics because of oncological safety. 4 years later, Kim and Han(2) presented video again to evoke modest impetus and critics tone was much down at that time because MIS has been accepted widely through successful way of a cholecystectomy in the mean time. Small group of young surgeons interested in LG strived to get adequate surgical skills and better instruments and devices. In the meantime, academic exchange between pioneering expertise Japanese surgeons opened surgical horizon widely. Uyama et al.(3) introduced fine dissection technique using ultrasonic shears and, Noshiro et al.(4) showed delicate dissection utilizing suction electrocautery dissecting instrument. In the year 2002, at least 10 young surgeons started newly developed style of laparoscopic gastrectomy. It was much nearer to radical surgery to be accepted as an option for early gastric cancer. Start was slow but, spread was so rapid after 2002 to initiate organizing study group and performing multicenter clinical study. Korean Laparoscopic Gastrointestinal Surgery Study (KLASS) group was started and activated in 2003. The achievements in laparoscopic surgery like the publication has increased since 1996, and international publication started from 2003 and the number of articles and sum of impact factor has continuously increased (Fig. 1, 2).
This review encompasses all achievements of Korean laparoscopic gastric surgeons in terms of international publication with high impact factor. Although, domestic publication and other activities is not included, tremendous effort for well performed study greatly contributed improving quality of life of the patients and treatment for gastric cancer.
The Dawning of the Laparoscopy Age (1996~2002)
After the first laparoscopy-assisted distal gastrectomy (LADG) for early gastric cancer was performed in 1991,(5) it has been performed in Korea since 1995. Choi et al.(6) first reported that six patients had been successfully performed LADG between September 1995 and February 1996. Yi et al.(7) first demonstrated that the LADG is superior to the open distal gastrectomy (ODG) regarding to the postoperative recovery, such as pain and hospital day. Sentinel lymph node (SN) biopsy in gastric cancer was started in Korea.(8)
The Rapid Penetration of LG (2003-2007)
Articles with impact factor and the concept of advancement of laparoscopy in gastric cancer had been published since 2003. First prospective randomized study for comparison of LADG and ODG in Korea demonstrated that LADG has a clear advantage over ODG in terms of resulting in fewer pulmonary complications while maintaining the curability of EGC.(9) In phase II clinical trial, Lee et al.(10) showed the feasibility of LADG in terms of similar compliance rate to ODG. Retrospective study showed perioperative recovery were faster in laparoscopy than in open surgery without difference of number of retrieved nodes, postoperative morbidities and mortality despite the longer operation of laparoscopy.(11)
Regarding the SN biopsy, detection rate was reported 90~94%.(12,13) Sensitivity in using both isotope and dye was 87.5% higher than that in using dye or isotope only.(12) However, SN biopsy was recommended cautiously because of SNs at the level II nodes.(13)
The learning curve regarding the operation time and the rate of complications reached the plateau after 30~50 cases of LADG.(14) Therefore, hand-assisted distal gastrectomy may be a bridge learning technique in laparoscopic gastrectomy.(15) High body mass index in female patients, old age, and male gender was found be risk factors of morbidity.(16)
The Period of Maturity (2008~2011)
Prospective randomized study about the comparison of the LADG and ODG first showed the improvement of the quality of life for up to 3 months in the LADG group regarding EORTC QLQ-30 and QLQ-STO 22 questionnaires.(17) Interim analysis of KLASS I trial showed that there was no significance difference in the morbidity and mortality between LADG and ODG groups.(18)
Retrospective study also demonstrated that despite the longer operation time, LADG group had lower complication rates and similar total number of retrieved lymph nodes comparing ODG group.(19) Overall morbidity and mortality rates were 14.0% and 0.6% in retrospective study.(20) Comorbidity, lack of experience, and degree of lymph node dissection were risk factors in studies.(20-22) There were no significant differences in postoperative morbidity or mortality between young and elderly group.(23) Regarding the high body mass index, there were no significant differences in postoperative complications except operation time.(24) Kang et al.(25) recommend that surgeons should pay attention to bleeding in Billroth I reconstruction and stump leakage in Billroth II reconstruction. The overall 5-year survival rate (95.5~96.9%) in LADG group was not significantly different from those in ODG group.(26,27)
Da Vinci system was introduced and used for operation of gastric cancer in 2005 in Korea. Song et al.(28) first reported that robot-assisted gastrectomy was found be safe and effective in treating early gastric cancer. Retrospective studies showed robot assisted gastrectomy was comparable to laparoscopy in terms of surgical and oncological outcomes despite of initial experience of robotic operation.(29-31)
LATG has been widely accepted and performed in early gastric cancer in this period. However, morbidity was 13.8~26.9% in LATG higher than in open total gastrectomy.(32) Various methods about esophagojejunostomy and lymph node dissection were investigated and found be feasible in LATG.(33,34)
In a porcine model, laparoscopic wedge resection or segmental resection with sentinel basin dissection first appears to be safe and technically feasible.(35) To improve the accuracy of SN mapping, Indocyanine green and (99m)Tc-tin colloid injections(36) and 2 mm thin slice frozen section and rapid immunohistochemistry were investigated.(37) Also high FOXP3+ Treg density of the SLN as a indepently significant predictor of non-SLN metastasis(38) and skip metastasis(39) were studied for false negative of SN biopsy.
Laparoscopy assisted function preserving gastrectomy such as the jejuna pouch interposition was tried and found be feasible and better in quality of life than conventional laparoscopy assisted gastrectomy.(40)
Conclusion
During the past 10 years, LG became a standard procedure in Korea through active learning, education, and academic communication. Well designed large scale powerful clinical studies are actively ongoing. International collaboration may further activate various valuable studies to develop minimal invasive gastric surgery for gastric cancer worldwide. Quality of life of the patients and safety of surgery would be improved further. Next goal must be to develop function preserving surgeries and selection of appropriate surgery for individual patients, to develop robotic surgery, computer-assisted visualization, and other electronic instruments more and simultaneously to reduce cost of surgery through technological innovation, and not to resist technology dependent surgery just because of medical cost.
 XML Download
XML Download