

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Lumbar ribs are persistent costal elements of the vertebrae that have failed to undergo the normal fusion and apoptotic changes consistent with costal elements in all normal non-thoracic vertebrae [123]. A review of literature reveals a global incidence of cervical ribs ranging from 0.04% up to 4.5% [4], intrathoracic ribs in about 50 cases to date [5] and very few reports on supernumerary ribs in the lumbar [367] and sacral regions [1] so rare that no consensus has been established on their incidence or prevalence rates. The presence of lumbar ribs may cause errors in enumerating the vertebral segments or levels on radiographs [2]. In addition, the cavity of the costotransverse joint between the supernumerary rib and the transverse process may be mistaken for a fracture of the transverse process of the lumbar vertebra on radiographic images [2]. Lumbar ribs are usually asymptomatic; however, a case of a lumbar rib causing pain and discomfort in the renal angle has been reported [7]. It is therefore important for clinicians and medical students to be aware of the anatomical variation in order to minimise misdiagnoses. The authors present a rare case of bilateral lumbar ribs articulating with the transverse processes of the first lumbar vertebra (L1).
Case Report
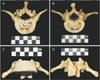
During a routine inventory of the research skeletal repository in the Raymond A. Dart Collection of Human Skeletons housed in the School of Anatomical Sciences, Faculty of Health Sciences, University of the Witwatersrand, a case of bilateral supernumerary ribs on the first lumbar vertebra (L1) was observed. The skeletal specimen belonged to a 70-year-old African male whose recorded cause of death was esophageal carcinoma. The entire vertebral column was well preserved and skeletonized. Vertebrae of the lower lumbar regions showed prominent lipping osteophytes and these were considered within normal limits for an individual at the recorded biological age. It was also noted that the first sacral vertebra (S1) was partially fused to the rest of the sacrum suggesting a case of lumbarization and an increase in the total number of free vertebrae. The first lumbar vertebra (L1) appeared complete with no deficiencies observed in any of its segments (Fig. 1). It demonstrated the typical characteristics of a medium sized kidney shaped body, triangular shaped vertebral foramen, and short quadrangular spinous process. A closer inspection from the inferior view revealed joint lines between the transverse processes and the supernumerary ribs on both sides (Fig. 1B). Plain radiographic imaging of the vertebra confirmed the existence of joint cavities between the transverse processes and the supernumerary lumbar ribs (Fig. 2A, B). Both ribs were approximately 4 cm in length and were significantly less than the total length of the 12th rib bilaterally. When viewed from the anterior aspect, the lumbar ribs followed an inferolateral course (Fig. 1C) whereas the superior and inferior views revealed a posterolateral course with slight anterior concavity such that the extremities of each rib were directed laterally (Fig. 1A, B). The ends of each rib were rounded and convex indicating the absence of associated costal cartilage or costochondral joints in vivo.
Ethical clearance was granted and covered by the Human Tissue Act (No. 65 of 1983) and the National Health Act (No. 61 of 2003), ethics number W-CJ-140604-1 on the use of human specimens for teaching and research.
Discussion
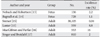
The first recorded case of human lumbar ribs was reported by Cumming in 1926 in which bilateral lumbar ribs articulated to the third lumbar vertebra (L3) were identified. Over the years isolated cases of lumbar ribs have been reported in relation to first lumbar vertebra (L1) [37] and the second lumbar vertebra (L2) [8]. No consensus exists on the incidence rates of lumbar ribs and the overview by Chernoff and Rogers [4] shows inconsistent figures ranging from 0.04% to as much as 16%. Incidence rates of lumbar ribs have been shown to vary between fetuses and adults (Table 1). The differences in the incidence rates in experimental animal models have been attributed in part to the comparisons of both embryos and adults. The significantly higher incidence rates in embryos are caused by the inclusion of ossification sites that will later disappear with ontogeny [4]. Lumbar ribs may be classified as either rudimentary if they are devoid of a cartilaginous end and their total length is less than half the total length of the twelfth rib or as extra ribs when they are considerably long and have cartilaginous ends [2910].
Development of lumbar ribs
Definitive thoracic ribs develop from the anteromedial sclerotome which migrate laterally as a costal process into the lateral body wall [4]. In other vertebral segments apart from the thoracic region, the costal processes will degenerate and partially fuse with the vertebral body to form the definitive transverse processes [124]. However, if the costal processes fail to degenerate they will develop into supernumerary ribs either in the cervical region or the lumbar region [124].
Development and differentiation of the axial skeleton as well as the positional identity of each somite along the cranio-caudal axis are under the control of the homeobox (Hox) genes [11]. Abnormalities in the expression of these genes have been associated with the occurrence of lumbar ribs, particularly the Hoxa10 gene which is expressed along the thoracolumbar junction [2911]. In cases where the cranial limit of Hoxa10 gene expression was displaced by one or two segments in the caudal direction, the first lumbar vertebra (L1) displayed phenotypic characteristics of thoracic vertebrae such as the persistence of costal processes, which later form lumbar ribs [29]. This is accompanied, in some cases, by lumbarization of the first sacral segment as depicted in the current study [1112]. Ectopic expression of Hox-c6 gene and mutations of the FYVE, RhoGEF, and PH domain-containing protein 1 (FDG1) gene or errors in its signaling pathway have also been implicated in lumbar rib development [9]. In addition, sodium salicylate and elevated level of maternal corticosteroids were also associated with the development of supernumerary lumbar ribs in both mice and rats [2411]. The current evidence suggests that the occurrence of supernumerary ribs could be an indication of teratogenic insult at a critical embryonic stage during ontogeny [911].
Clinical manifestations
Lumbar ribs are usually detected as incidental findings during routine radiographic imaging of the lumbar region. Unlike cervical ribs, which have been implicated in vascular and neurological abnormalities of the superior thoracic aperture, the majority of cases of lumbar ribs have been asymptomatic. However, in one case of the lumbar rib was associated with pain in the left renal angle [7]. Furthermore, due to their rarity, lumbar ribs have often been mistaken for kissing osteophytes, abdominal vessel abnormalities, and/or fractures of the transverse processes [37]. Lumbar ribs may also present a significant challenge during percutaneous renal biopsy through the renal angle between the twelfth rib and the first lumbar vertebra (L1) [3].

 XML Download
XML Download