

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Primary hyperparathyroidism is the most frequent cause of hypercalcemia, and its prevalence is increasing due to the routine examination of serum calcium levels. Primary hyperparathyroidims is most commonly caused by an adenoma or hyperplasia of the parathyroid gland. A cystic parathyroid adenoma is an extremely rare cause of primary hyperparathyroidism.
In our case, a-79-year old female presented with lower back pain and constipation. Her serum calcium, phosphate and immunoreactive parathyroid homone levels were 15.6, 1.8 mg/dL and 371.8 pg/mL, respectively. Neck CT revealed a cystic mass and a contour bulging heterogeneous mass in the left inferior right thyroid gland, respectively. These mass lesions were removed, and the intra-operative parathyroid hormone levels monitored, to confirm the complete resection. After removing the left cystic mass to the inferior thyroid, the serum calcium and immunoreactive parathyroid hormone levels quickly returned to normal.
We report a case of primary hyperparathyroidism, caused by a cystic parathyroid adenoma, with a brief review of the literature.
Figures and Tables
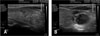
Fig. 1
Neck sonogram shows complicated cystic mass in the inferior pole of the left thyroid gland and heterogenous, slightly echogenic mass in the inferior pole of the right thyroid gland.



References
2. Turner a, Lampe HB, Cramer H. Parathyroid cysts. J Otolaryngol. 1989. 18:311–313.
3. de Ridder VA, Brom HL, Blok P. Hyperparathyroidism due to primary cystic parathyroid adenoma. Neth J Surg. 1986. 38:134–137.
8. Higgins CB. Role of magnetic resonance imaging in hyperparathyroidim. Radiol Clin North Am. 1993. 31:1017–1028.
9. Clark OH. Parathyroid cysts. Am J surg. 1978. 135:395–402.
10. Albertson DA, Marshall RB, Jarman WT. Hypercalcemic crisis secondary to a functioning parathyroid cyst. Am J Surg. 1981. 141:175–177.
11. Mitchell BK, Kinder BK, Cornelius E, Stewart AF. Primary hypeparathyroidism: preoperative localization using technetium-sestamibi scanning. J Clin Endocrinol Metab. 1995. 80:7–10.
12. Ginsberg J, Young JEM, Walfish PG. Parathyroid cysts: Medical diagnosis and management. JAMA. 1978. 240:1506–1507.
13. Pacini F, Antonelli A, Lari R, Gasperini L, Baschieri L, Pinchera A. Expected parathyroid cysts diagnosed by measurements of thyroglobulin and parathyroid hormone concentration in fluid aspirates. Ann Int Med. 1985. 102:793–794.
14. Irvin GL, Dembrow VD, Prudhomme DL. Clinical usefulness of an intraoperative "quick parathyroid hormone" assay. Surgery. 1993. 114:1019–1022.
15. Howe JR. Minimally invasive parathyroid surgery. Surg Clin North Amy. 2000. 80:1399–1426.
16. Mandl F. Therapeutisher versuch bein falls von ostitis fibrosa generalisata mittles: extirpation eines epithelkorperchen tumors. Wien Klin Wochenshr Zentral. 1926. 143:245–284.
17. Mitmaker B, Lerman S, Lamoureus E, Begin L. Parathyroid cyst: diagnosis and treatment of an unusual surgical problem. Can J Surg. 1991. 34:59–61.
18. Okamura K, Ikenoue H, Sato K, Yoshinari M, Nakagawa M, Kuroda T, Fujishima M. Sclerotherapy for benign parathyroid cysts. Am J Surg. 1992. 163:344–345.
 XML Download
XML Download