

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Asthma is a heterogeneous disease. The phenotypes of asthma are classified according to both clinical and pathological factors. Since chronic airway inflammation is a fundamental feature of asthma, categorizing patients based on their inflammatory cells has also been emphasized.
To evaluate airway inflammation, invasive methods such as bronchial biopsy and bronchoalveolar lavage have been applied to asthmatic patients [1]. However, bronchoscopy is not only potentially hazardous but also hard to perform. Therefore, noninvasive methods for assessing airway inflammation have been employed, and analyzing induced sputum is the most commonly used test for asthma.
The simple and practical classification of asthma involves 2 categories: eosinophilic asthma (EA) and noneosinophilic asthma (NEA). In addition, 4 subtypes have also been proposed—eosinophilic, neutrophilic, paucigranulocytic, and mixed cellularity—depending on the presence or absence of sputum eosinophilia and neutrophilia [2]. Although the exact clinical implications for each inflammatory asthma phenotype should be further clarified, identifying these phenotypes may be useful in clinical practice, particularly for the eosinophilic subtype that is usually a good predictor of response to corticosteroids [34]. Furthermore, many novel biologics for severe asthma target the eosinophilic phenotype by blocking the cytokines that are directly linked to eosinophilic infiltration, such as interleukin (IL)-4 [5], IL-5 [6789], and IL-13 [10111213].
When interpreting the results of induced sputum analysis, there are several factors that can influence cellular profiles. Most importantly, corticosteroid-based medications are potentially critical since they could contribute to increased airway neutrophilia [14] and reduced eosinophilia [15]. Moreover, there is the possibility that the inflammatory cellular phenotypes for each patient do not remain stable over time.
Determination of the inflammatory phenotype before starting medications in newly diagnosed asthmatic patients helps to predict response to certain therapeutic options. However, there certainly exists an unmet need of evaluating the profiles of asthmatic patients on maintenance therapy in order to provide insights into the clinical course of the disease and modulate asthma medications according to the results of the sputum analysis. Nevertheless, repetitive sputum analysis is not routinely performed in clinical practice, nor has the stability of airway inflammatory patterns been extensively explored. Only a few studies have investigated, and the results of these reports are controversial [21617181920].
In our current study, we investigated if inflammatory subtypes are stable over time in patients with stable asthma and evaluated the differences in the clinical characteristics between groups that demonstrate different longitudinal transition patterns in terms of their sputum inflammatory cell profiles.
MATERIALS AND METHODS
Study patients and design
A total of 149 asthmatic patients (>18 years) receiving inhaled corticosteroids (ICS) who had undergone sputum analysis twice at the out-patient clinic of a tertiary referral hospital were included. The interval between the 2 induced sputum examinations varied among the patients (mean, 29.6 months; 95% confidence interval, 26.74–32.47). During the interval, patients have taken ICS and other asthma medication regularly.
All of the patients were diagnosed with asthma based on either the presence of airway hyperresponsiveness (provocative concentration of methacholine causing a 20% fall in forced expiratory volume in 1 second [PC20] < 16 mg/mL on methacholine bronchial provocation test) or positive bronchodilator test according to the American Thoracic Society criteria. All patients were clinically stable without asthma exacerbation at the moment of sputum examination. Patients with any symptoms of respiratory infection within 4 weeks before sputum examination, other pulmonary diseases, or significant comorbidity were excluded. This study was approved by the Institutional Review Board of Asan Medical Center (approval number: 2014-0971) and obtained signed informed consent from all patients.
All patients were subjected to a detailed retrospective review. Demographic data and various clinical information, such as atopic status, age at asthma onset, duration of asthma, ICS treatment duration, compliance, asthma control status, results of the pulmonary function tests, PC20 values, blood eosinophil counts, total IgE, and the results of the induced sputum analysis, were obtained at both sputum examinations. Before sputum induction all subjects were asked to fil up in a self-administered asthma control test questionnaire. Patients were evaluated adherence to ICS by using count of inhaler prescribed according to the medical records, overall clinical judgment of physician, and inhaler technique assessment. An individual's baseline compliance to ICS (range, 1–3) was based on count of inhaler prescribed according to the medical records, overall clinical judgment of physician, and inhaler technique assessment before the sputum induction; higher scores denote more compliance.
The data were analyzed and compared between the phenotypes and study groups that were classified according to the results of the induced sputum analysis, as described below.
Sputum induction and analysis
Sputum was induced using aerosolized 0.9% saline, followed by a 3%–5% NaCl solution through a nebulizer [21]. Patients were asked to blow their nose, rinse their mouth, and swallow water to minimize contamination by postnasal drip and saliva. The expectorated sputum was processed according to the protocol previously described [22]. The slides were stained with Giemsa, and differential cell counts were expressed as the percentage out of nonsquamous cells. Those with significant squamous cell contamination (>80%) were excluded from further analyses [23].
Classifications of the sputum inflammatory cellular patterns
A sputum eosinophil percentage ≥3% was used to define eosinophilic inflammation. The normal range for the sputum eosinophil count was determined using the cutoff point for the 95th percentile used to define healthy control groups [2]. A sputum neutrophil percentage ≥40% was considered neutrophilic inflammation as referenced by a previous report [24].
Based on these criteria, patients were divided in 2 different ways: (1) Patients were classified into 4 phenotypes—eosinophilic, neutrophilic, mixed granulocytic, or paucigranulocytic inflammation—by the eosinophil and neutrophil counts; and (2) Patients were divided into 2 phenotypes—EA or NEA—according to the presence of eosinophilic inflammation, regardless of the presence or absence of sputum neutrophilia.
Subjects with sputum neutrophil proportion ≥40% and <3% sputum eosinophil proportion were classified as neutrophilic inflammation and those with an eosinophil proportion ≥3% and <40% neutrophils were classified as eosinophilic inflammation. Subjects had both increased neutrophils and eosinophils and were classified as mixed granulocytic inflammation. A further group had normal levels of both neutrophils and eosinophils were classified as paucigranulocytic inflammation.
The eosinophilic phenotype consists of all subjects with more than 3% eosinophils; eosinophilic inflammation + the mixed granulocytic inflammation. And noneosinophilic phenotype consists of all subjects with less than 3% eosionphils; neutrophilic inflammation + the paucigranolocytic inflammation.
In addition, we also divided the patients into 4 groups according to the transition patterns of their sputum profiles: group 1, eosinophilic to eosinophilic phenotype; group 2, eosinophilic to noneosinophilic phenotype; group 3, noneosinophilic to eosinophilic phenotype; and group 4, noneosinophilic to noneosinophilic phenotype.
Statistical analysis
The results for the continuous variables were expressed as the mean ± standard deviation. Categorical data were reported using frequencies and percentages. The Kruskal-Wallis test was used to assess the different subgroups of patients with asthma. The Spearman rank correlation coefficient was used to assess the association between the blood cell counts and sputum cell counts. Results were considered significant when p < 0.05. Data analysis was performed using IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA).
RESULTS
Comparison of the clinical characteristics of different asthma phenotypes, as defined using sputum eosinophils and neutrophils
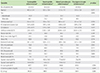
The proportions of each inflammatory phenotype at the initial sputum examination were as follows: eosinophilic inflammation (n = 32, 21.5%), neutrophilic inflammation (n = 35, 23.5%), mixed granulocytic inflammation (n = 53, 35.6%), and paucigranulocytic inflammation (n = 29, 19.5%). There was no significant difference in the clinical characteristics between the 4 phenotypes (Table 1).
At the second sputum examination, asthmatic patients were again divided into 4 phenotypes: EA (n = 17, 11.4%), neutrophilic asthma (n = 58, 38.9%), mixed granulocytic inflammation (n = 59, 39.6%), or paucigranulocytic inflammation (n = 15, 10.1%). The clinical features of the 4 inflammatory phenotypes also demonstrated no significant differences.
Next, we compared the clinical characteristics of EA and NEA at the time of both sputum examinations. At the initial sputum examination, EA comprised 57.0% (n = 85) and NEA comprised 43.0% (n = 64) of the study population. At the second sputum examination, EA comprised 51.0% (n = 76) and NEA comprised 49.0% (n = 73). EA demonstrated a significantly higher level of blood eosinophils. There were no significant differences in other clinical characteristics between EA and NEA patients, as shown in Tables 2. No differences were observed for ICS treatment duration (EA, 4.96 ± 6.43 years; NEA, 4.89 ± 6.02 years), ICS dose or compliance to ICS therapy.
There was a significantly positive relationship between the blood eosinophil counts and percentage of sputum eosinophils (r = 0.536, p < 0.001 at the initial examination; and r = 0.594, p = 0.002 at the second examination).
Clinical characteristics of 4 groups defined by the different transition patterns of the sputum inflammatory cell profiles
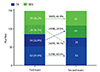
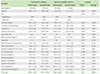
The changes in the sputum eosinophil and neutrophil counts between the first and second sputum examinations were remarkably variable (Fig. 1). The proportions of the each group were 34.9% (n = 52), 22.8% (n = 34), 16.1% (n = 24), and 26.2% (n = 39) for groups 1, 2, 3, and 4, respectively. The percentage of the patients who demonstrated sputum profile transition reached 39.9% of all patients (58 of 149 patients). Thirty-four of the initially EA patients (39.5%; 34 of 86 patients) were NEA at their second sputum examination. Twenty-four of the initially NEA patients (38.1%; 24 of 63 patients) demonstrated eosinophilic airway inflammation at the follow-up examination (Fig. 2). The initial blood eosinophil counts were significantly higher in group 1, which demonstrated persistent sputum eosinophilia, in comparison with the other groups. No other significant differences in the clinical features or laboratory findings obtained at the initial examination were found among the 4 groups. No differences were observed for ICS treatment duration, ICS dose or compliance to ICS therapy and forced expiratory volume in 1 second predicted level at the second examination among the four groups (Table 3).
DISCUSSION
In our study, a substantial number of asthmatic patients demonstrated certain sputum inflammatory cellular patterns that transitioned over time, in clinically stable settings. No factors other than blood eosinophil counts were found to predict persistence or changes in certain types of airway inflammatory patterns.
Defining asthma phenotypes is pivotal for implementing individualized treatments to each asthmatic patient. Clearly, the airway inflammatory pattern in steroid-naïve asthmatic patients could provide valuable information for determining the future clinical course and responsiveness to treatment. In particular, airway eosinophilia is a good predictor of response to inhaled steroids [3] and the likelihood of benefiting from higher doses of systemic corticosteroid treatment [4]. Trials that used sputum eosinophil percentages to guide treatment and predict asthma control report positive results [81017252627]. Furthermore, many novel biologics for severe asthma target eosinophilic phenotypes. On the other hand, trials that used sputum neutrophils to manage refractory asthma have reported mixed effectiveness of antibiotics [282930]. Considering the clinical importance of the inflammatory patterns of asthma, defining airway inflammation phenotypes is pivotal for managing asthma patients. Despite the clinical usefulness of sputum examination for determining inflammatory phenotypes, it is unclear if the results of induced sputum analyses alone are sufficient and reliable for determining the true phenotypes.
Our results demonstrated a wide range of percentages for the sputum eosinophils and neutrophils, and more than half of all patients (n = 85, 57.0%) had eosinophilic inflammation, although all of our study patients were quite clinically stable and receiving the appropriate ICS treatment. Interestingly, various clinical parameters demonstrated no significant difference between eosinophilic and NEA as classified according to the results of the induced sputum analysis. These results suggest that the classification of airway inflammatory phenotypes in stable asthmatic patients receiving ICS may not significantly anticipate different clinical courses or prognoses. The phenotypes that were classified before ICS treatment would be more important for predicting the prognosis of asthma. In our study, appropriate ICS therapy was maintained for all subjects throughout the 2 study visits and, therefore, the possibility of the steroid medication effect on modulating airway inflammation may be excluded. However, it is still possible that treatment with ICS abolishes the intrinsic airway inflammatory pattern in asthmatic patients.
In this study, we evaluated if inflammatory phenotypes are stable over time in the patients with stable asthma and the results were found quite unstable. These results are consistent with the findings of several other studies. One earlier study reported an inconsistency between sputum inflammatory profiles over 5 years [2]. Another prospective study on patients with moderate to severe asthma revealed that the inflammatory phenotype was unstable [16]. Also in line with our current findings, a recent study on the Pan-European BIOAIR cohort found that allocation to clusters changed in 42.3% of patients when stratified according to airway inflammation. This instability has been also found in steroid-naive asthmatic patients. In one study, repeated sputum analyses were performed for the patients not receiving ICS and the results demonstrated that 22% had persistent eosinophilia, 31% had eosinophilia on ≥1 occasion, and 47% had persistent noneosinophilia [19]. Another study has reported that 35% of steroid-naive asthmatics demonstrated changes in their inflammatory phenotypes [18]. Moreover, phenotypic variability was reported that it is not influenced by changes in the corticosteroid dose [17]. In contrast, another study reported that the majority of adult patients with difficult-to-treat asthma demonstrated consistent sputum analysis results over a 5-year period and that the percentage of sputum eosinophils was highly reproducible [20]. The inconsistent findings from the different studies described above might be due to the small number of patients, differences in asthma severity, possible effects of varying doses of corticosteroid therapy, and variable confounding factors such as exposure to tobacco smoke. Taken together, the evidence suggests that various factors possibly influence airway inflammation and the potential variability of the inflammatory patterns should be considered when defining inflammatory phenotypes in asthmatic patients. This also indicates that the inflammatory cell type alone is not sufficient to predict treatment outcomes.
Finally, we attempted to determine if there were any unique characteristics of the groups that showed inflammatory phenotype transitions. Only few studies have investigated the clinical factors affecting airway inflammatory pattern transition in asthma and one study has reported that there were no clinical differences between the different inflammatory patterns [17]. In our study, interestingly, a high blood eosinophil count was the only factor for predicting the sustainability of EA, and no other clinical differences were found. The blood eosinophil count has been reported to exhibit good correlation with sputum eosinophils in asthmatic patients [31], which is associated with disease severity and asthma phenotypes [3233]. Blood eosinophils can be used to predict and direct anti-inflammatory therapy, for which there is preliminary evidence for asthma [89]. A recent study reported that using a cutoff value of 0.45 × 109 cells/L for blood eosinophilia can usefully predict airway eosinophilia in patients with severe asthma [34]. In another study of mild to moderate asthma, as well as severe asthma, blood eosinophils demonstrated the highest accuracy for identifying sputum eosinophilia. The blood eosinophil count can be used as an easy-to-measure biomarker for sputum eosinophil percentage in patients with asthma, and can also have practical advantages for guiding novel anti-inflammatory therapies [35]. On the other hand, a recent study by the Severe Asthma Research Program demonstrated poor correlations between blood and sputum eosinophils [36], thereby raising controversy. Since blood eosinophils generally transmigrate quickly into tissues in response to localized inflammation, the association between the blood eosinophils and airway inflammation can be transient [37] and may lack strong positive correlation [36]. Although the correlation between the magnitude of blood eosinophils and airway eosinophilia could be modest, it can be clearly assumed that the use of blood eosinophils facilitates the individualized treatment and management of asthma.
The limitations of our study include the fact that the data were retrospectively analyzed so that the overall asthma control status could not be clearly defined and the time interval between the 2 sputum examinations was variable. Furthermore, it was hard to evaluate the clinical implications of each airway inflammatory pattern on the long-term clinical courses by using only our current findings. Prospectively designed studies with more frequent sputum eosinophil measurements are needed to verify our results and elucidate the meaning of each inflammatory cell transition in asthmatic patients. Another limitation was the relatively small number of study participants. It will be important in the future to include larger patient cohorts and undertake prospective analyses to determine the possible mechanism of phenotype instability in asthmatic patients.
In conclusion, a substantial proportion of asthmatic patients who demonstrate certain sputum inflammatory cell profiles at the initial examination will develop profile transitions over time in clinically stable settings. The results of our present study suggest that a single sputum sample assessment cannot reliably distinguish between EA and NEA and may not help guide clinical decisions in asthmatic patients. Further prospective studies are needed to search for valuable clinical factors to improve asthma management plan for inflammatory phenotype-based therapeutic strategies.


 XML Download
XML Download