

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Vertebral collapse after a trivial injury in elderly patients with severe osteoporosis, associated with severe back pain and vertebral fractures, is a common clinical problem.
Although osteoporosis is the most common cause of vertebral fractures in elderly patients, the spine is also one of the most common sites of metastatic disease, accounting for up to 39% of all bony metastasis.15)
Magnetic resonance (MR) imaging is helpful in determining the exact cause of vertebral collapse using morphologic and signal intensity criteria.
However, in the clinical setting, malignant spine metastasis can be difficult to differentiate from acute osteoporotic compression fracture, especially in cases with an accompanying trivial injury. Here, we present a confusing case of malignant metastasis misdiagnosed as acute osteoporotic compression fracture.
Case Report
A 78-year-old man was referred to our emergency department for the evaluation of low back pain and progressive weakness of the left lower limb. The patient had undergone percutaneous vertebroplasty at the L3 level with the diagnosis osteoporotic compression fracture 4 months earlier after a minor fall, and he had received a foraminotomy at the L3–4 level for foraminal stenosis 2 months before admission.
Neurological examination showed motor weakness of left knee extension, grade III. Routine hematological and serum chemistry tests, including erythrocyte sedimentation rate and C-reactive protein, yielded normal results.
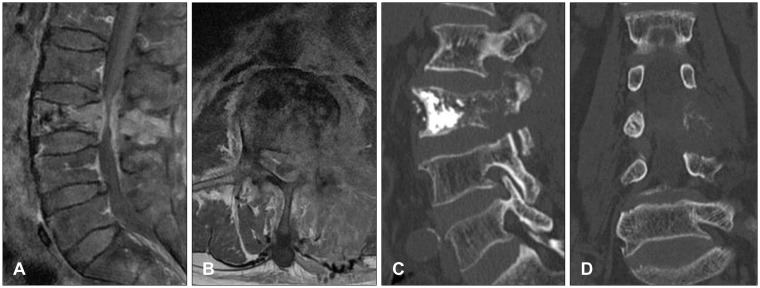
Gadolinium-enhanced MR images taken on the day of transfer showed increased signal intensity from the vertebral body to the posterior element (Figure 1A and B). An enhanced soft tissue mass in the left side of the L3 vertebral body was also observed. Computed tomography scan taken in the emergency department showed significant osteolytic change from the body to the pedicle (Figure 1C and D).
On the basis of the findings of typical pathologic compression fracture, emergent decompressive laminectomy of L3 and bone biopsy were performed including spinous process and vertebral body via left side pedicle. Histological evaluation confirmed metastatic squamous cell carcinoma.
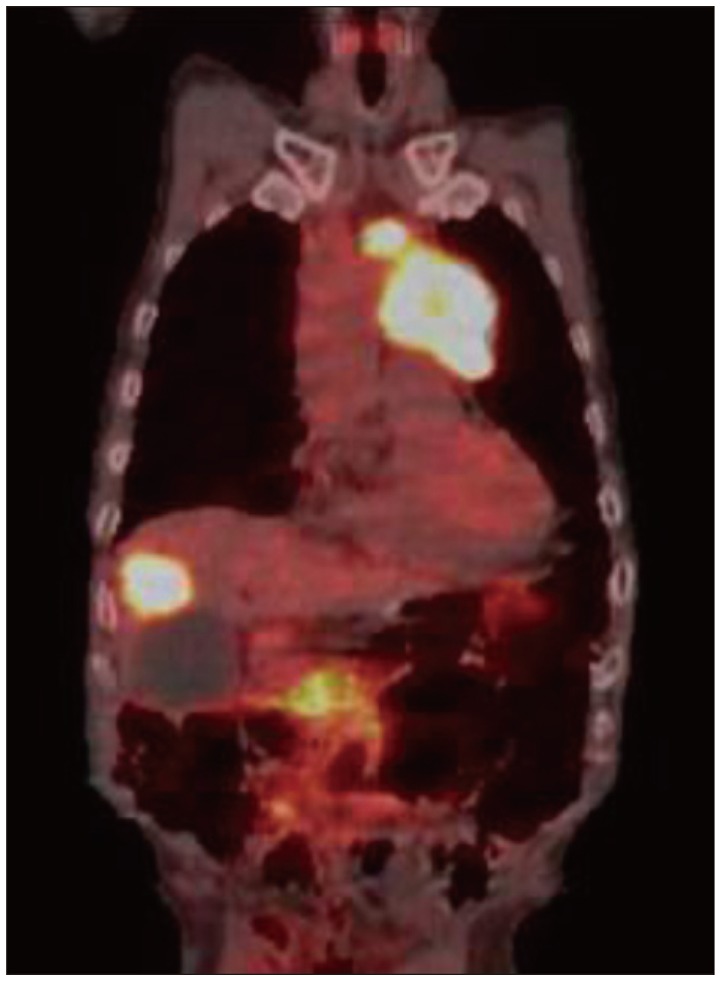
The patient was transferred to the hemato-oncological department for adjuvant treatment and further diagnosis. He was diagnosed as having squamous cell carcinoma of the lung on the percutaneous biopsy with hepatic and spine metastasis (Figure 2).
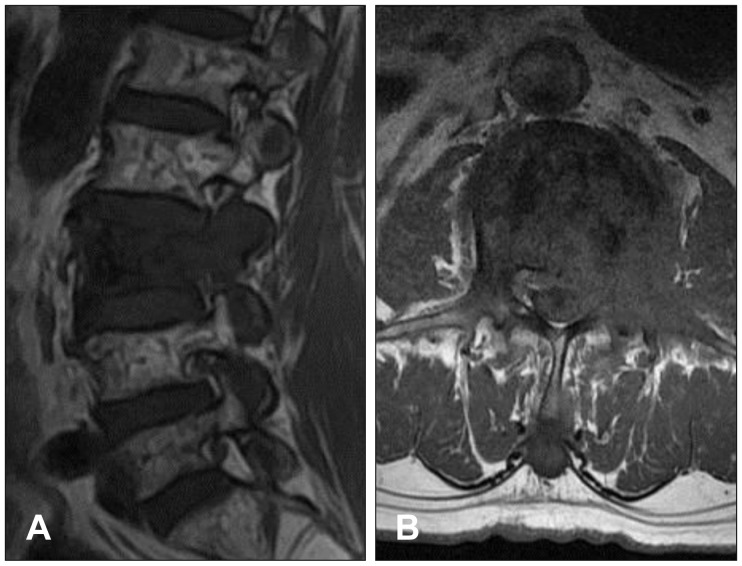
In the retrospective review of MR images taken 2 months (Figure 3) and 4 months (Figure 4) previously, obvious facet and pedicle involvement, and paraspinal soft tissue extension were noted. We believe that the doctors in the spine clinic should have suspected malignant metastasis and they should have investigated the radiological images more carefully during the patient's first visit.
Discussion
Differentiation between benign osteoporotic compression fractures and malignant pathologic fractures is clinically important, particularly in elderly patients with severe osteoporosis; however, it can be difficult.
Although several recent studies have applied new MR techniques in assessing vertebral collapse, routine evaluation of vertebral collapse commonly uses conventional spin-echo MR imaging.279)
Benign osteoporotic compression fracture is a common disease in elderly patients. Conventional spin-echo MR imaging findings suggestive of acute osteoporotic compression fracture include low-signal-intensity band on T1-weighted imaging (WI) and T2-WI, spared normal bone marrow signal intensity of the vertebral body, retropulsion of a posterior bone fragment, and multiple compression fractures.3)
On the other hand, MR imaging findings suggestive of metastatic pathologic fracture include a convex posterior border of the vertebral body, abnormal signal intensity of the pedicle or posterior element, epidural mass, encasing epidural mass, focal paraspinal mass, and other spinal metastases.6)
Among the various findings suggesting malignant pathologic fractures or benign compression fracture, pedicle involvement is controversial. Yuh et al.8) compared the conventional spin-echo MR imaging findings between 84 benign fractures and 25 malignant fractures on T1-WI and T2-WI. They reported pedicle involvement in 22 of the 25 patients with malignant compression fractures but in none of 52 nontraumatic compression fractures. Therefore, involvement of the pedicle is an important clue for the diagnosis of malignant pathologic fractures.
However, Ishiyama et al.4) reported that pedicle involvement, which had been accepted as a common indicator of malignant processes, was also frequent in patients with osteoporotic compression fractures, particularly in the early phase, and was not specific for malignancy on new MR techniques, such as short inversion time inversion recovery (STIR) and gadolinium-enhanced T1-WI.
In this case, some clinical and MR imaging data may have misled the doctors of the local spine clinic to the diagnosis of benign compression fracture at L3, including the clinical history of minor trauma and severe osteoporosis based on bone mineral densitometry. Moreover, they performed conventional MR examination, as most spine doctors do.
In the retrospective review of T1- and T2-weighted MR imaging findings, it was determined that the obvious left pedicle involvement in the image taken 4 months previously and the aggravation of the pedicle and facet with paraspinal soft tissue mass at L3 in the image taken 2 months earlier were highly suggestive of malignancy.
The spine clinicians had better to suspect malignant metastasis from the beginning, in case of pedicle involvement on T1, T2 and fat suppression view although they did not perform STIR or gadolinium-enhanced MR imaging.
Conclusion
Although differentiating between benign compression fractures and malignant pathologic fractures is possible in most cases, a diagnosis of malignant pathologic fracture should be assumed when there is an obvious pedicle involvement. In case of ambiguity, further tests should be performed for an exact diagnosis, including bone biopsy or short-term MR imaging follow-up.

 XML Download
XML Download