

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Despite recent advances in the care for the acute traumatic brain injury, it remains a lethal lesion. Contralateral hematoma after decompressive surgery for acute traumatic brain injury, where the brain is usually tense, is uncommon.2781014) Delayed hematoma, contralateral hematoma, alternating hematomas, or bilateral hematomas are other terms used to describe this entity.7) An immediate postoperative diagnosis and therapeutic intervention are of extreme importance if a new hematoma forms on the side contralateral to the acute traumatic brain injury because it is a possible lethal condition if unrecognized.14) We present our experience of these patients and discuss the diagnosis and management.
Materials and Methods
Study design
Twelve patients with acute traumatic brain injury who developed a delayed contralateral hematoma after evacuation of an acute hematoma from April 2008 to March 2014 were included. Clinical and radiographic information was obtained through a retrospective review of the medical records and radiographs. Furthermore, we divided the patients into less severe (Glasgow Coma Scale [GCS] score >8) and severe (GCS <8) injury groups for analysis.
Clinical data
By retrospective review of the medical records, we collected the demographic data, the head injury mechanism, neurological status, operative findings and method, and clinical course. The neurological status included the GCS score. Functional outcome was evaluated at discharge using the Glasgow Outcome Scale (GOS) score: death (Death; grade 1), persistent vegetative state (PVS; grade 2), severe disability (SD; grade 3), moderate disability (MD; grade 4), good recovery (GR; grade 5).
Radiographic data
The type and location of primary and contralateral hematoma, presence of a skull fracture and brain swelling overlying the contralateral site, and Marshall grade were reviewed. Marshall Grade divides patients depend on computed tomography (CT) abnormalities in brain trauma; Grade 1 (normal CT scan), Grade 2 (cisterns intact and midline shifting less than 5 mm), Grade 3 (citerns compressed or absent and midline shifting less than 5 mm), Class 4 (midline shifting more than 5 mm).5) Brain swelling was measured in the preoperative CT as the distance from the midline to the septum pellucidum; brain swelling was diagnosed when the mean midline shift was >1 cm.
Results
Ten males and two females were included. Mean age was 44.3 (range, 9-65) years. Mean admitting GCS score was 6.17 (3-10). Ten (83.3%) patients presented with a severe injury (GCS <8), and the others (16.7%) had moderate injuries. Five (41.7%) patients had suffered a traffic accident (TA) involving at car or as a pedestrian. Four (33.3%) were admitted for a falling injury. Three (25%) were admitted for rolling or slipping.
The initial main diagnoses were five (41.7%) subdural hematomas (SDHs), five (41.7%) epidural hematomas (EDHs), and four (33.3%) intracerebral hematoma (ICH), and one (8.3%) subarachnoid hematoma. The contralateral-side hematoma that formed after the acute hematoma in was an EDH in eight (66.7%), a SDH in two (16.7%), and an ICH in three (25.0%). According to the initial preoperative Marshall grade, one patient was rated 2, five were rated 3, and six were rated 4. The postoperative Marshall grade distribution was two patients were 2, 4 patents were 3, and six patients were 4.
The initial CT scan revealed 10 supratentorial hematomas and two infratentorial hematomas. Nine (75%) patients had a skull fracture on the contralateral side of the acute hematoma on a CT scan, and eight (83.3%) patients had brain swelling.
Seven (70%) of the 10 patients in the severe head injury group and the two (100%) patients in the less severe injury group had skull fractures on the contralateral side of the acute hematoma. Brain swelling was seen in eight (80.0%) patients in the severe head injury group and two (100%) in the less severe injury group.
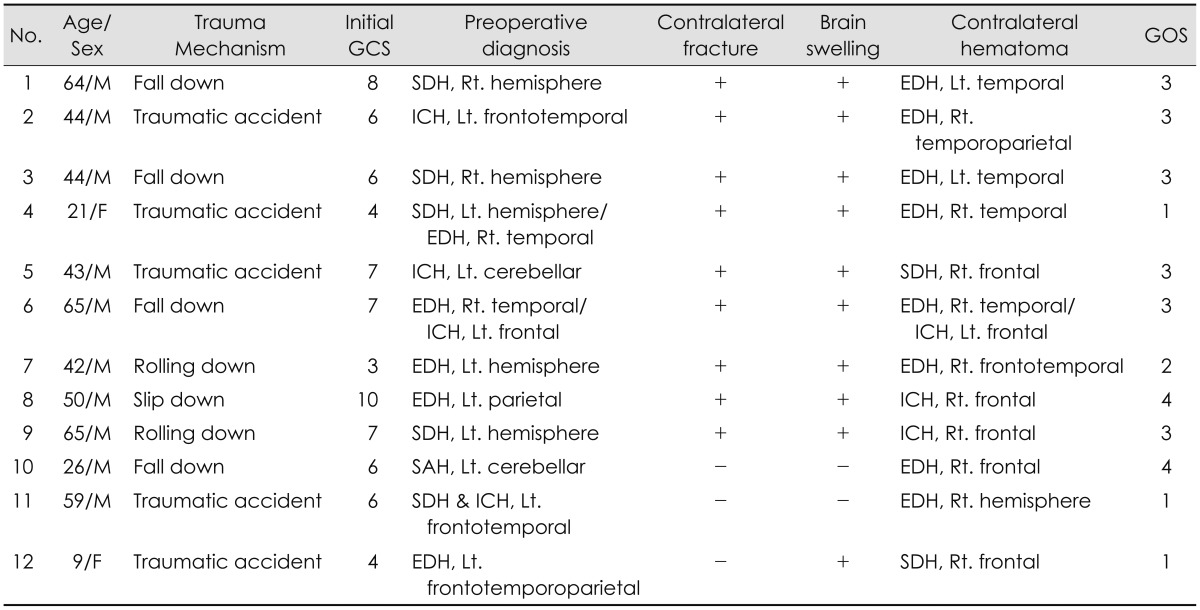
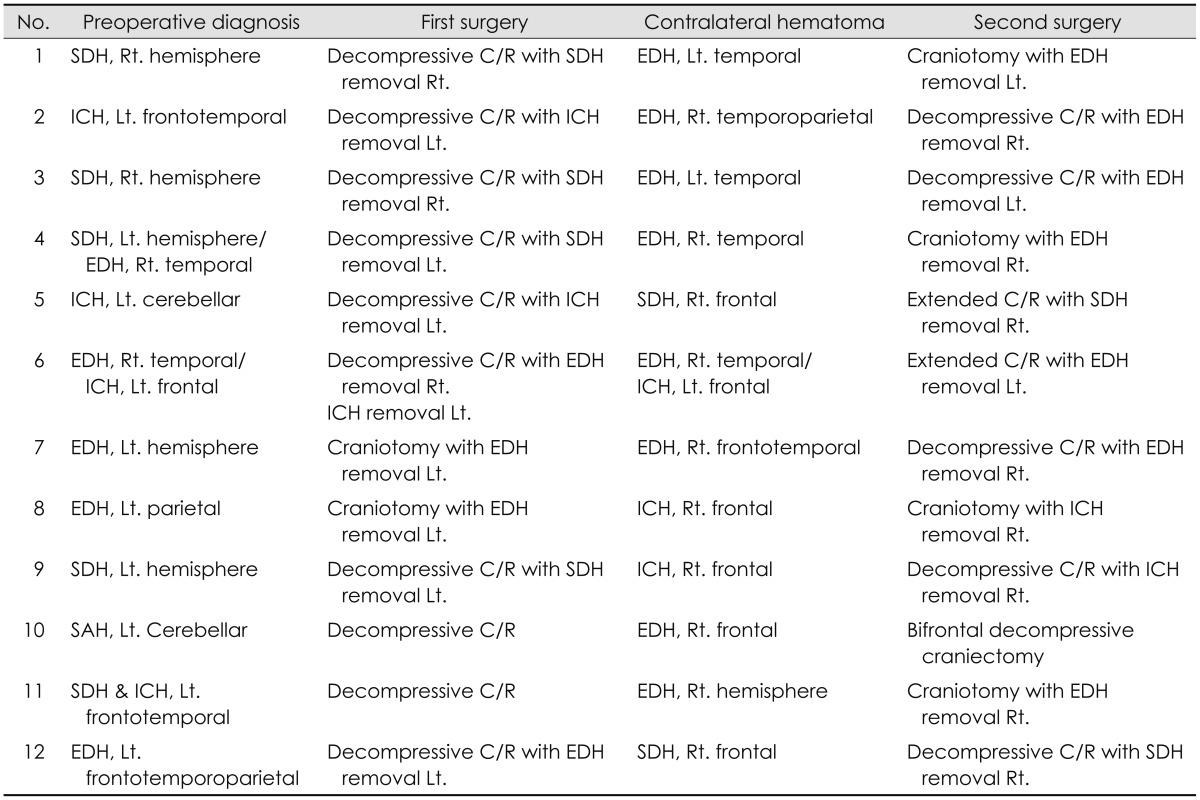
Patient outcomes according to the GOS score at follow-up were: two (16.7%) patients had MD; six (50.0%) had SD; one (8.3%) was in PVS; and three (25.0%) had Death. There were 4 complicated cases. Three (25.0%) were sepsis and one (8.3%) was pneumothorax. The clinical and radiographic data of these patients are summarized in Table 1 and 2.
Illustrative case
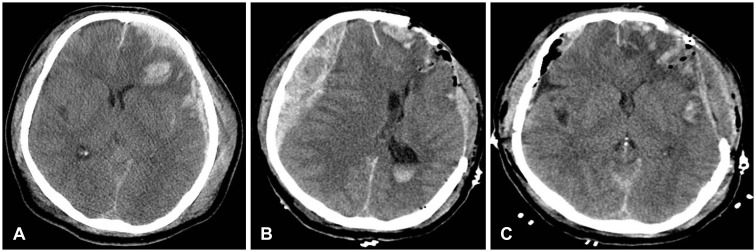
A 59-year-old man without known systemic disease presented in our emergency department with complaints of mental deterioration after traumatic accident. His initial GCS score was 7 (Eye opening: 2, Verbal: 2, Motor response: 3), and CT of the brain revealed SDH over the left frontal cerebral surface (Figure 1A). Emergency decompressive craniectomy and hematoma removal was performed, and during surgery there was no significant brain swelling. The postoperative CT showed newly developed EDH on the contralateral side with midline shifting over 2 cm (Figure 1B). Secondly, emergency craniotomy and hematoma removal was performed (Figure 1C). But one day after operation, the patient was expired.
Discussion
Delayed development of a contralateral EDH after evacuating an acute SDH is rare.461315) However, many neurosurgeons have experienced such cases. Several neurosurgical procedures are associated with the incidence of contralateral hematoma, including evacuating an acute or chronic SDH and inserting a ventriculo-peritoneal shunt.10) Moreover, the development of a contralateral hematoma at the evacuation site of an acute SDH or EDH is also rare.7) Authors have reported various incidence rates (very rare to 5.7%) of contralateral hematoma after evacuating an ipsilateral hematoma.2681014) In our study, the initial diagnoses of the patients were six (50%) SDH, four (33.3%) EDH, and two (16.7%) CH.
Contralateral hematomas can appear without any clinical status change.1114) However, intraoperative brain swelling, postoperative neurological deterioration, pupillary dilation contralateral to the SDH, grand mal seizure, and intractably elevated intracranial pressure (ICP) are suggestive of new hematoma formation.1014) If the brain swells even after completely removing a SDH, neurosurgeons almost always suspect the development of a contralateral EDH.4) In this study, intraoperative brain swelling was seen in ten (83.3%) patients.
A contralateral skull fracture is the highest risk factor for a delayed hematoma development.7) Moreover, contralateral fracture indicates the possibility of a tear in dural vessels, but without obvious collection of extra-axial blood due to the tamponade effect.7) The fracture can be easily detected on a bone CT or a good quality plain radiograph.7) In our study, a skull fracture on the contralateral side of the acute hematoma was noted on the CT scans of nine (75%) patients, especially, six (50%) were EDH. Therefore, in case of a contralateral side skull fracture, the surgeon should be alert to the possibility of the postoperative contralateral EDH development.7) In case of contralateral developed SDH and ICH, all four cases showed intraoperative brain swelling, and three showed contralateral skull fracture. In operation, there were no specific findings which can predict contralateral SDH or ICH. According to Park et al.9) excessive or too fast evacuation of hematoma can be a contralateral SDH developing factor. And An and Jwa1) hypothesized that sudden increase of cerebral flow after decompression with defective autoregulation can be cause of contralateral ICH.
Several reasons have been proposed for delayed hematoma formation, including tamponade effect loss, a vasomotor mechanism, and coagulopathy.7) It has been hypothesized that the initial impact causes a contrecoup injury as well as a coup injury with a skull fracture and bleeding from the dura mater or fracture site.14) On the other hand, the mass effect from a contrecoup hematoma increases the ICP and produces a tamponade effect at the contralateral bleeding source, preventing formation of a hematoma.1214) So, some authors have reported precipitating factors of contralateral hematoma such as surgical decompression, cerebrospinal fluid fistula, increase of the ICP control, and systemic hypotension.210) Nevertheless, the ICP should be decreased in patients with a severe mass effect and brain stem compression, despite of the possible risk of a delayed contralateral hematoma.
Immediate diagnosis may overturn the poor outcome in these patients.14) The diagnosis of the possible contralateral hematoma is controversial. Some authors have proposed explorative burr holes trephination over the fracture during the first surgery.10) However, we prefer to take a CT scan before any such exploration, as the utility of blind exploration is doubtful.7) A CT scan readily delineates the size and location of a contralateral hematoma, dictates the therapy, and can detect other intracranial lesions.1014) Previous studies indicate that the formation of hematoma in a traumatized brain is a dynamic process and is best monitored by serial CT scans.711) Intraoperative ultrasound can also be helpful for detecting any new lesion during surgery.3) However, intraoperative imaging tools may not always be available and growth of other hematomas is a rare phenomenon.4) We recommend a CT scan to detect hematoma immediately after hemicranial decompression, which helps in timely detection and treatment.
In this study, ten (83.3%) patients with severe injury (GCS <8); two (16.7%) showed MD, six (50%) severe disability; one (8.3%) were in a PVS; and three (25%), died. However, contralateral hematoma evacuation has potential value for improving the prognosis in these patients, unless they have impaired brain stem sign.14) Therefore, contralateral hematoma should be evacuated promptly if it produces a significant mass effect, to facilitate improvement in patients.
There are some limitations in this study. First, the number of patients was small. Second, since this study was a retrospective study, it could only analysis limited clinical findings correlations. We think that prospective multicenter study is needed.
 XML Download
XML Download