

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The physiological balance of sera in neurocritical patients can be easily destroyed after a major surgery such as decompressive craniectomy. The course of coagulopathy due to major bleeding during and after the surgery would accelerate the imbalance of acid-base equilibrium of our blood.16) Biomarkers such as arterial pH, standard base excess (SBE), and lactate have been well-known for its predictive power of mortality and morbidity.92527)
During the medical management of such traumatic patients, the complex fluctuation of the electrolyte states in the sera is another concern to bear in mind. For example, of many electrolytes, chloride is one of our body's principle ions and it represents 70% of the total negative ion content. 4) It is an important extracellular anion in charge of maintaining acid-base balance and movement of water in our body. However, compared to other major ions such as sodium, hyperchloremia has somewhat been neglected. The recommended guideline of fluid therapy for traumatic brain injury (TBI) is the use of isotonic sodium chloride solutions (0.9% saline solution).35) Normal saline has a high chloride content of 154 mmol/L when the normal serum chloride concentration is 100 to 110 mmol/L. The overuse of continuous intravenous infusion of 0.9% saline solutions may resultantly cause hyperchloremic metabolic acidosis, which brings about other side effects such as coagulopathy due to hemostatic changes.28) During the course of treating the TBI patients, the changing patterns of all these factors eventually reflect the evolving conditions of the patients. The vicious cycle of imbalance of acid and base will lead to a poor outcome of post-operative patients with high morbidity and mortality.212324)
To our best knowledge so far, there has been no clinical article reporting the relationship between the patterns of biochemical markers and mortality of the patients with decompressive craniectomy specifically. This study is the first attempt in analyzing the predicting factors of mortality in decompressive craniectomy by investigating the data obtained from routine clinical tests during the management at intensive care unit (ICU).
Materials and Methods
Patients
This is a retrospective study of 96 patients with acute subdural hematoma (SDH). All these patients underwent urgent decompressive craniectomy between January 2014 and December 2015. Of 147 cases of decompressive craniectomy with acute SDH, 96 patients were included for final analysis. Fifty-one of the patients were excluded because they had missing laboratory variables or because they stayed in the ICU less than 24 hours. The study was approved by the Institutional Ethics Committee. Because the laboratory tests and data collected in this study are part of routine clinical practice, informed consent from the patient was waived.
Baseline demographics
The clinical parameters for the analysis of this particular group of patients were as follows: age, gender, medical history (e.g., hypertension, diabetes mellitus), initial blood pressure, initial pulse rate, need for mechanical ventilation, operation time, intra-operative blood loss, length of ICU stays (days), pre-operative and post-operative arterial blood gas analysis (e.g., pH, SBE, bicarbonate, PaCO2, lactate) electrolytes (sodium, chloride, anion gap), complete blood count (CBC) with hemoglobin, white blood cells, and platelet counts, serum creatinine, and serum albumin. The data was retrieved from the electronic clinical database.
Laboratory tools for serum analysis
The laboratory tools used in our institution are as follows: 1) arterial blood gas analyzer (RAPIDLab 1265; Siemens Healthcare Diagnostics Inc., Tarrytown, NY, USA); 2) CBC (ADVIA2120i, Siemens Healthcare Diagnostics Inc.); and 3) chemical electrolyte analyzer (VISTA 1500; Siemens Healthcare Diagnostics Inc.). According to our machine, the normal range of the concentration of serum chloride is 98 to 107 mmol/L. Above 107 mmol/L will be defined as hyperchloremia.
Statistical analysis
Data are expressed according to the properties of the variable. Continuous variables are presented as mean and standard deviation. Categorical variables are presented as frequency and percentage. In order to compare two groups, we performed the two-sample t-test or chi-square test (Fisher's exact test) as appropriate. Logistic regression analysis was used to identify the factors that effected to mortality and the results are presented as odds ratio (OR) with 95% confidence interval (CI). The area under the receiver-operating characteristic curve (AUC), which distinguishes between survivors and non-survivors of each model was also measured and compared. A p-value less than 0.05 was considered statistically significant and all statistical analyses were conducted using SAS 9.4 version (SAS Inc., Cary, NC, USA).
Results
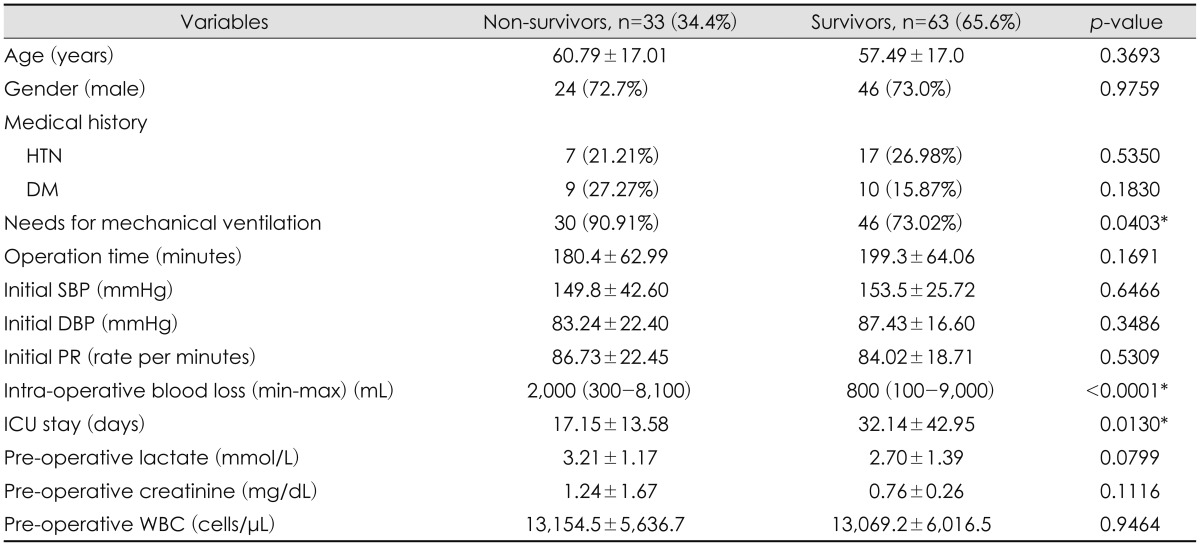
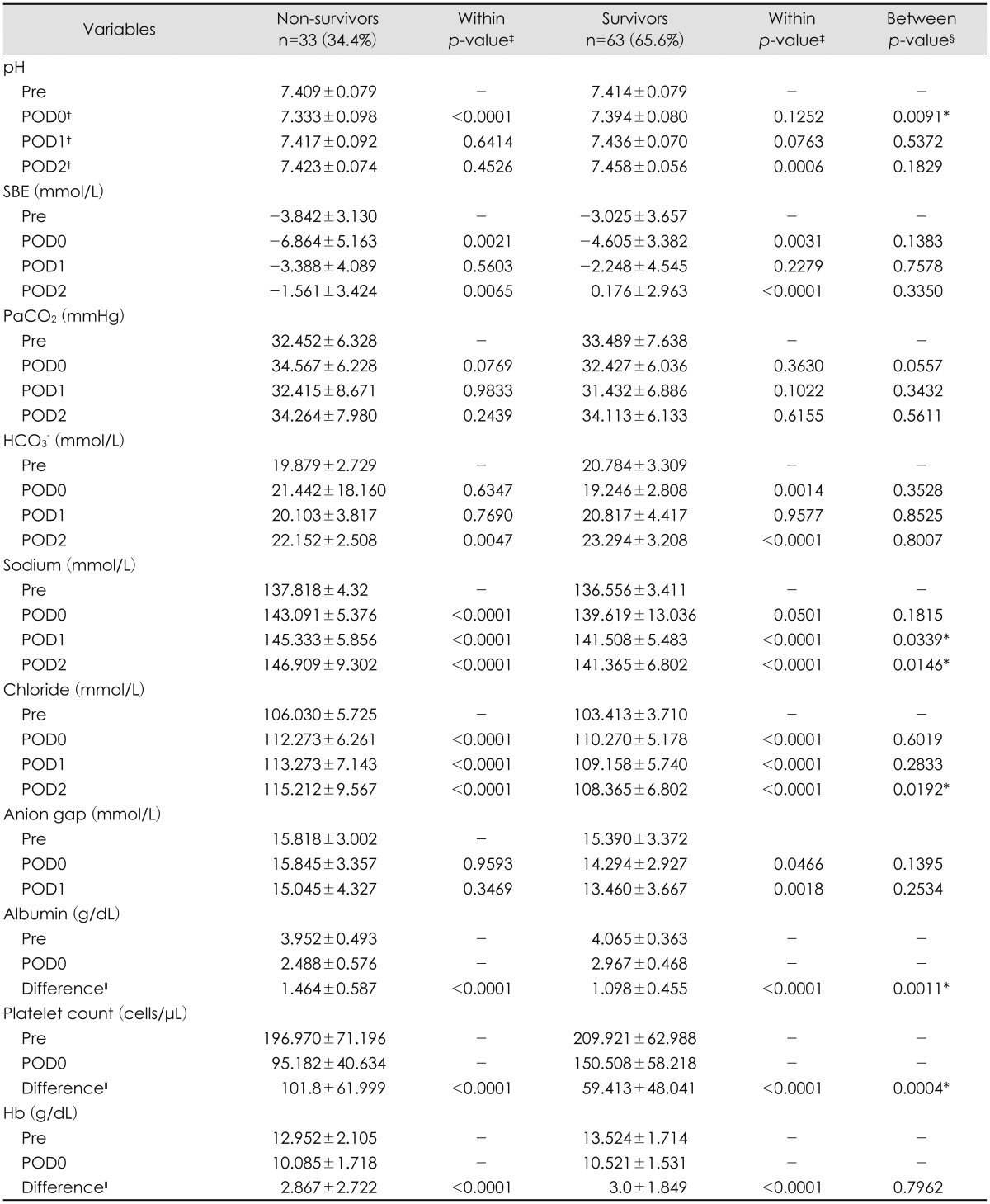
Ninety-six patients with acute SDH, who underwent decompressive craniectomy, were analyzed in this study. The demographic and clinical variables of the patients associated with mortality are shown in Table 1 and 2. The comparison between survivors and non-survivors in hospital showed a statistical difference in the following parameters: needs for mechanical ventilation, a large amount of intra-operative blood loss, and shorter length of ICU stays (Table 1). The average difference of measurements between pre-operative and post-operative albumin and platelet count on post-operative day (POD) 0 was statistically significant not only within the survivors but also within the non-survivors (p<0.0001 and p<0.0001, respectively). The average difference of arterial pH between pre-operative and POD 0 measurements was statistically significant (p<0.0001) within the non-survivors. However, it was not statistically meaningful within the survivors (p=0.1252). The average difference of arterial pH between the groups of survivors and non-survivors showed a statistical significance only on POD 0 (p=0.0091) (Table 2).
The average difference of measurements between pre-operative and post-operative sodium and chloride on POD 1 and POD 2 was statistically significant not only within the survivors but also within the non-survivors (p<0.0001 and p<0.0001, respectively). On POD 2, serum sodium and chloride concentrations measured 48 hours after decompressive craniectomy were increased significantly that there was a statistical difference to discriminate the survivors and non-survivors (p=0.0146 and p=0.0192, respectively) (Table 2).
Table 3 presents the results of the multivariate logistic regression. In this model, the average difference in pre-operative and POD 0 albumin, and that in pre-operative and POD 0 platelet counts were independently associated with mortality (p=0.0247 and p=0.0067, respectively). Moreover, the average difference in pre-operative and post-operative serum chloride measured on POD 2 was also strongly related with mortality (p=0.0158).
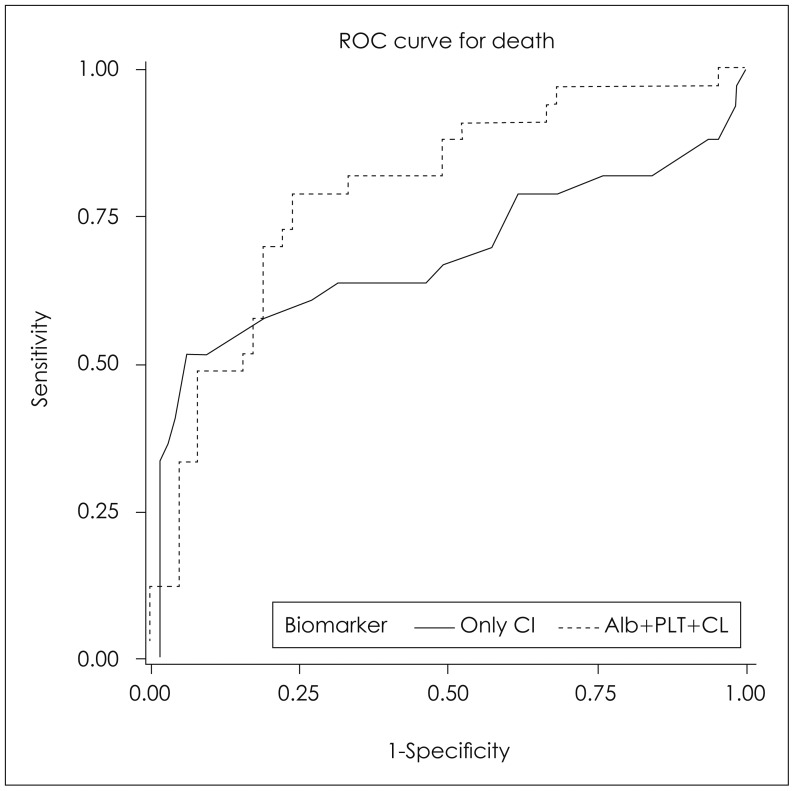
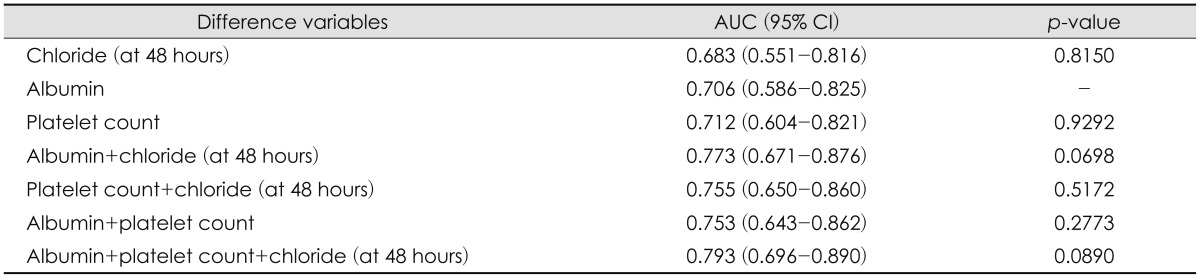
Interestingly, according to our data in Table 4, individual variable is not distinctively powerful to predict in-hospital mortality of the patients with decompressive craniectomy. The pre-operative and POD 2 differences in serum chloride (48 hours after surgery) alone gave an AUC of 0.683 (95% CI, 0.551-0.816). However, the multiple logistic regression model combining albumin, platelet count and chloride (48 hours after surgery) together gave an AUC of 0.793 (95% CI, 0.696-0.890) (Table 4). In this final model, we discovered that the combination of data eliciting the pre-operative and post-operative differences in albumin and platelet count on POD 0, and differences in pre-operative and POD 2 serum chloride were independently associated with mortality. Meanwhile, the isolated values of each parameter were less powerful to predict mortality. The AUC model with chloride alone (AUC=0.683) and the model combining albumin, platelet count on POD 0, and serum chloride on POD 2 (AUC=0.793) were compared in Figure 1. Unfortunately, p-value for this model was not statistically significant (p=0.0890). Yet, we believe that this data in Table 4 still has its worth to draw an attention in representing a good clinical discrimination between survivors and non-survivors when we only compare the absolute values of AUC between the chloride alone and the combined model of albumin, platelet count, and serum chloride (AUC=0.683 vs. AUC=0.793, respectively). The combined factors significantly improved the model.
Discussion
Our retrospective analysis with 96 patients with decompressive craniectomy is based on the study of a subset of acutely critical patients, where the situations with pre-operative and post-operative hypoperfusion and hypoxia would eventually lead to an inevitable death in some victims regardless the rigorous surgical and medical resuscitation. Of numerous clinical parameters, the authors considered that the biochemical markers of serum are the most abundant sources in quickly assessing the survivorship of the TBI patients in the acute settings of trauma management.
The demographic profiles of our patients showed that a large amount of blood loss during decompressive craniectomy, the needs for mechanical ventilation and a shorter length of ICU stays were the key clinical parameters of non-survivors (Table 1).
TBI has long been known for its association with coagulopathy.1529) Even if the amount of blood loss is not voluminous, the brain injury itself is a cause of coagulopathy in many trauma patients although the pathophysiology is yet poorly understood among the neurosurgeons.29) As our data suggested, a large amount of blood loss would worsen the pro-coagulant state of the TBI patients. Additionally, this vicious cycle of coagulopathy is consequently linked with hyperchloremic metabolic acidosis, post-operative thrombocytopenia, and hypoalbuminemia, henceforth, leading to a poor outcome with mortality. The physiological aspect of biochemical markers in predicting mortality with decompressive craniectomy will be discussed in more detail in the later part of this section.
The needs for mechanical ventilation and shorter length of ICU stays are other clinical factors of mortality in patients with decompressive craniectomy. Surviving neurosurgical patients tend to have a longer ICU and in-hospital stays.2) This is also usually associated with longer ventilator time.2) This phenomenon of poor survivorship with the needs for mechanical ventilation and shorter ICU stay is ironically explained that the injury of patients were so severe that he or she was not able to endure the lethal process of secondary injury even after undergoing decompressive craniectomy.714)
In conjunction with the clinical factors of poor survivorship mentioned above, the biochemical measurements of serum in the TBI patients are our great interests in hoping that these will aid to identify the patients with higher mortality. The epidemiology of TBI patients with decompressive craniectomy is complex. The factors of pre-hospital and in-hospital care as well as the predisposing morbidities (e.g., cardiovascular disease, liver dysfunction, renal failure) of individual patients affect the final outcome of the TBI patients.19) Different clinical states of patients are correlated with the biochemical measurements of serum. The physiological acid-base conditions and the hemodynamic states of the patients are shown in the laboratory findings and these can be monitored and corrected, if required. The laboratory data in the acute phase of patients with decompressive craniectomy were evaluated in this study. In attempting to account for the role of acidosis, we confirmed that the initial arterial pH on POD 0 is an important factor in discriminating survivors and non-survivors (Table 2). Kaplan and Kellum13) investigated the acid-base variables in major vascular injury and their study supports our findings. The variables with acidosis such as arterial pH on POD 0 are strong factors to distinguish between survivors and non-survivors.
Our data also showed that post-operative hyperchloremia seemed to be quite common in the patients who underwent decompressive craniectomy. Our analysis showed that there is an association between the post-operative hyperchloremia and in-hospital mortality after decompressive craniectomy (Table 2 and 3). The survivors and non-survivors both had high serum chloride concentration >107 mmol/L on POD 1 and POD 2 (Table 2). Serum sodium levels were also elevated with a statistical significance. Hyperchloremia has been reported to be associated with mortality in non-neurosurgical cases and the issues of incorrect fluid therapy were mentioned.212324) One of the major factors that will partially dictate the acid-base and electrolyte balance is a regimen of fluid therapy in managing neurocritical patients.18) The indifferent infusion of normal saline during and after the neurosurgical operation may have a link with post-operative hyperchloremia. Our data was more focused on the average differences in the measurements of pre-operative and POD 2 serum chlorides. The authors thought that this reflects the real-time clinical situation. The isolated values of each biochemical measurements are important. However, the "patterns" of those values are more relevant and critical in delineating the in situ state of the clinical condition. Thus, we thought that this was one of authentic methods in predicting mortality in the patients with decompressive craniectomy.
Fluid therapy is another aspect in changing the physiological state of the body in an acute trauma setting. This has a close link with transfusion protocols. Normal saline is usually recommended for transfusion of red blood cells by Korean blood agencies; hence, a massive transfusion with isotonic saline containing high concentrations of chlorine may aggravate the hyperchloremic state. In the situation with trauma-induced massive active bleeding with disruptions in hemostasis, coagulopathy will be combined to worsen the patient prognosis.615) As mentioned previously, TBI on its own is a high risk factor for coagulopathy due to a rerelease of tissue factors leading to disseminated intravascular coagulation. Transfusion is inescapably associated with platelet dysfunction. Thrombocytopenia after TBI is documented in many articles.122) When there is a platelet dysfunction immediately after the surgical treatment, this may further increase the bleeding risks of the patients. Our data showed that all these circumstances including post-operative thrombocytopenia may attribute to a higher risk of mortality after decompressive craniectomy. However, it is worthy of note that there is a separate issue of controversial debate whether platelet transfusion is beneficial in preventing mortality of cerebral hemorrhagic patients.817)
Lastly, albumin is well-known to be a strong predictor of survival.1012) It has many roles such as anticoagulant effects.20) Hypoalbuminemia is mainly known to occur due to albumin loss during the massive bleeding and due to the process of hemodilution during the fluid resuscitation.20) Post-operative hypoalbuminemia was observed in the non-survivors of decompressive craniectomy in our study. Together with metabolic acidosis by hyperchloremia, acid-base balance is disrupted when the blood content is diffusely interrupted with massive fluid therapy and transfusion during the stressful operation.112026) Hypoalbuminemia has its unique stance as a strong predicting factor of mortality in the patients with decompressive craniectomy (Table 3).
According to our data, the combined prognostic model of post-operative hyperchloremia, thrombocytopenia, and hypoalbuminemia, reflecting the differences in the pre-operative and post-operative measurements, is a potential tool to predict the survivorships of decompressive craniectomy after TBI (Table 4).
Limitations
The nature of this study is retrospective and the number of patients included is rather small. A lack of information on the fluid resuscitation and administration prior to the emergency operation should be considered as the pre-operative fluid therapy may have some influences in the post-operative conditions. The pre-operative evaluation on the severity of TBI was not intensively considered in this study because the main focus was on the analysis of the post-operative risk factors of mortality in a subset of patients with decompressive craniectomy. However, future study should accommodate the pre-operative neurological states of the patients to systematically analyze the independent factors of mortality.
This clinical analysis was the first attempt to apply the trends in the differences of serologic measurements of the pre-operative and post-operative clinical variables in attempting to discover good parameters of discrimination between the survivors and non-survivors in decompressive craniectomy.
Conclusion
This study was conducted to show the changing patterns of the patient condition, which are reflected in the timely differences of measurements in the serum biomarkers. Knowing that the isolated values of laboratory data is static in its nature, the authors demonstrated the originality of this study by analyzing the trends in the pre-operative and post-operative serologic data of serum chloride, platelet counts and albumin in order to assess the survivorships of this particular subset of patients. The physiological disturbances in the acid-base balance and hemodynamic instability with coagulopathy before and after the neurosurgical operation are detrimental. A combined prognostic model of differences in the measurements of hyperchloremia, thrombocytopenia, and hypoalbuminemia were strongly associated with increased mortality in the patients with decompressive craniectomy.

 XML Download
XML Download