

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Accidents with a pneumatic nail gun, which has been used in the construction industry, have increased.2) However, reports on management of a patient with a nail gun injury to the cranium are rare. The authors report on a case of a patient treated with simple retraction after small skin and prophylactic antibiotic administration.
Case Report
A 56-year-old man had five nail gun-shots due to attempted suicide and was transferred to the emergency room. On his physical examination, his mental status was drowsy and there was no neurological deficit except for nails on his cranium. In his past history, there was no psychological background, however, he used to drink often and became depressed.
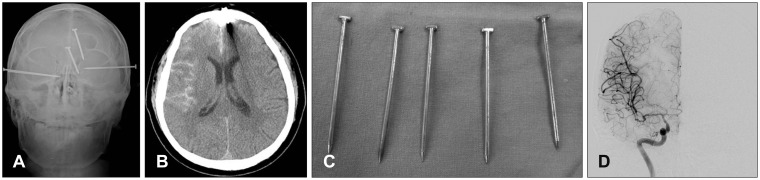
On plain skull radiography, five nails were found (Figure 1A). Among the five nails, two penetrated glabella. Two nails were located in the right parietal bone and another was located in the left parietal bone. Due to the head of the nail, the direction was confined to the outer table of the skull. In addition, a subarachnoid hemorrhage was observed on brain computed tomography (CT)(Figure 1B). No involvement of major arteries or sinuses was found on CT angiography.
All procedures were performed in the operating room under general anesthesia in order to treat the emergent condition as rapidly as possible. The nail head was located beneath the scalp and tightly attached to the skull, it was not visible from the outside. A small incision to advance a forceps and a rongeur was necessary, and then the nail head was extracted easily without resistance. In the same manner, all nails were removed successfully (Figure 1C). During the period of conservative management, there was no cerebrospinal fluid leakage or symptoms or signs of infection. Antibiotics including vancomycin, ceftriaxone, and metronidazole were administered for two weeks and carbamazepine was administered for a week. Conventional angiography was performed, and there was no vascular invasion or newly formed fistula (Figure 1D). The patient was discharged without complication.
Discussion
Head injury by pneumatic nail gun injury is rare, and there have been some case reports on management, treatment. According to Lee and Park,4) the speed of the launched nail and presence of the nail head are important determinants of the extent of nail gun related head injuries. If major artery or sinuses are not involved, extraction from the nail head could be the main treatment.
CT is typically the first-line radiologic examination in the emergency room for head-injured patients. In general, CT shows excellent details in bone and average value in soft tissue. Failure to recognize cerebral damage following penetrating brain injuries, especially when there is retained foreign body, can lead to serious life-threatening complications.1) In addition, because involvement of the large vessels is critical to determining the operative strategy, vascular integrity should be evaluated with CT angiography or CT enhanced image in the initial evaluation in the emergency room. In this case, nails were removed by a small scalp incision due to the fact that major artery or sinuses were not involved. If this is not the case, management would be direct ligation or vascular bypass surgery.
Despite many controversies regarding use of prophylactic antibiotics, the authors believe that broad spectrum antibiotics are appropriate for patients with penetrating brain injury since these wounds are considered to be contaminated. It is also recommended that antibiotics should be started as soon as possible.3)
Post-traumatic epilepsy is a major cause of disability and inadequate social integration. Although there is no prospective study to indicate the efficacy of prophylactic anti-epileptic medication following a traumatic brain injury, it has been recommended that patients be covered for about the first week after injury with a medication such as phenytoin or carbamazepine.5)
Conclusion
In the patient with head injury by pneumatic nail gun, the first evaluation should focus on the shape of the nail head and vascular integrity from simple X-ray and CT. If the nail head is confined to the depth of skull penetration, cautious extraction of the nail head can be performed without postoperative complication and early start of prophylactic antibiotics can be the next treatment.
 XML Download
XML Download