

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Hypoxic-ischemic encephalopathy (HIE) is one of the major disease for neuro-rehabilitation, as well as one of the important impairment. HIE typically shows global deterioration of brain function with relative preservation of brain stem reflexes, and topographic pattern of damage; the CA1 hippocampal cells, cerebellar Purkinje cells, neocortical neurons in layers 3, 5, 6 and basal ganglia. The characteristics of patho-mechanism including persistent vegetative state, seizure, autonomic dysfunction and secondary Parkinsonism are causative factors of several complications. Management of these complications sometimes curative, but more often re-adaptive and palliative. Understanding and proper rehabilitation of complications will be one of the most important therapeutic strategies for patients with HIE.
Figures and Tables
Fig. 1
Rostral-caudal deterioration of brain function and the hypothetical relationship between duration of ischemia and resultingbrain damage.2
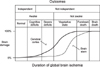

Fig. 3
Sample status epilepticus treatment algorithm for adults.15 IV: intravenous, ED: emergency department, IM: intramuscular, O2: oxygen, HR: heart rate, BP: blood-pressure, EKG: electrocardiogram, CBC: complete blood count, BMP: basic metabolic profile, Ca: calcium, Mg: magnesium, PO4: phosphate, LFT: liver function test, ABG: arterial blood gas, AED: antiepilepticdrug, HCG: human chorionic gonadotropin, PE: phenytoin equivalent, EEG: electroencephalogram.




References
1. Kaplan PW. Electrophysiological prognostication and brain injury from cardiac arrest. Semin Neurol. 2006; 26:403–412.
2. Khot S, Tirschwell DL. Long-term neurological complications after hypoxic-ischemic encephalopathy. Semin Neurol. 2006; 26:422–431.
3. Greer DM. Mechanisms of injury in hypoxic-ischemic encephalopathy: implications to therapy. Semin Neurol. 2006; 26:373–379.
4. Plum F, Posner JB, Hain RF. Delayed neurological deterioration after anoxia. Arch Intern Med. 1962; 110:18–25.
5. Petito CK, Feldmann E, Pulsinelli WA, Plum F. Delayed hippocampal damage in humans following cardiorespiratory arrest. Neurology. 1987; 37:1281–1286.
6. Foreman B, Hirsch LJ. Epilepsy emergencies: diagnosis and management. Neurol Clin. 2012; 30:11–41. vii
7. Lu-Emerson C, Khot S. Neurological sequelae of hypoxicischemic brain injury. NeuroRehabilitation. 2010; 26:35–45.
8. The Multi-Society Task Force on PVS. Medical aspects of the persistent vegetative state (2). N Engl J Med. 1994; 330:1572–1579.
9. Dougherty JH Jr, Rawlinson DG, Levy DE, Plum F. Hypoxic-ischemic brain injury and the vegetative state: clinical and neuropathologic correlation. Neurology. 1981; 31:991–997.
10. Physicians AroawpotRCo. The vegetative state: guidance on diagnosis and management. Clin Med. 2003; 3:249–254.
11. Levy DE, Caronna JJ, Singer BH, Lapinski RH, Frydman H, Plum F. Predicting outcome from hypoxic-ischemic coma. JAMA. 1985; 253:1420–1426.
12. Brain Resuscitation Clinical Trial I Study Group. Randomized clinical study of thiopental loading in comatose survivors of cardiac arrest. N Engl J Med. 1986; 314:397–403.
13. Krumholz A, Stern BJ, Weiss HD. Outcome from coma after cardiopulmonary resuscitation: relation to seizures and myoclonus. Neurology. 1988; 38:401–405.
14. DeLorenzo RJ, Pellock JM, Towne AR, Boggs JG. Epidemiology of status epilepticus. J Clin Neurophysiol. 1995; 12:316–325.
15. Hirsch LJ, Gaspard N. Status epilepticus. Continuum (Minneap Minn). 2013; 19:767–794.
16. Jumao-as A, Brenner RP. Myoclonic status epilepticus: a clinical and electroencephalographic study. Neurology. 1990; 40:1199–1202.
17. Baguley IJ. Autonomic complications following central nervous system injury. Semin Neurol. 2008; 28:716–725.
18. Fernandez-Ortega JF, Prieto-Palomino MA, Garcia-Caballero M, Galeas-Lopez JL, Quesada-Garcia G, Baguley IJ. Paroxysmal sympathetic hyperactivity after traumatic brain injury: clinical and prognostic implications. J Neurotrauma. 2012; 29:1364–1370.
19. Perkes I, Baguley IJ, Nott MT, Menon DK. A review of paroxysmal sympathetic hyperactivity after acquired brain injury. Ann Neurol. 2010; 68:126–135.
20. Baguley IJ, Heriseanu RE, Cameron ID, Nott MT, Slewa-Younan S. A critical review of the pathophysiology of dysautonomia following traumatic brain injury. Neurocrit Care. 2008; 8:293–300.
21. Baguley IJ. The excitatory:inhibitory ratio model (EIR model): An integrative explanation of acute autonomic overactivity syndromes. Med Hypotheses. 2008; 70:26–35.
22. Do D, Sheen VL, Bromfield E. Treatment of paroxysmal sympathetic storm with labetalol. J Neurol Neurosurg Psychiatry. 2000; 69:832–833.
23. Levy ER, McVeigh U, Ramsay AM. Paroxysmal sympathetic hyperactivity (sympathetic storm) in a patient with permanent vegetative state. J Palliat Med. 2011; 14:1355–1357.
24. Venkatesan A, Frucht S. Movement disorders after resuscitation from cardiac arrest. Neurol Clin. 2006; 24:123–132.
25. Eltahawy HA, Saint-Cyr J, Giladi N, Lang AE, Lozano AM. Primary dystonia is more responsive than secondary dystonia to pallidal interventions: outcome after pallidotomy or pallidal deep brain stimulation. Neurosurgery. 2004; 54:613–619. discussion 619-621.
26. Ghika J, Villemure JG, Miklossy J, Temperli P, Pralong E, Christen-Zaech S, Pollo C, Maeder P, Bogousslavsky J, Vingerhoets F. Postanoxic generalized dystonia improved by bilateral Voa thalamic deep brain stimulation. Neurology. 2002; 58:311–313.
27. Sage JI, Van Uitert RL. Man-in-the-barrel syndrome. Neurology. 1986; 36:1102–1103.
28. Duggal N, Lach B. Selective vulnerability of the lumbosacral spinal cord after cardiac arrest and hypotension. Stroke. 2002; 33:116–121.
29. Montero J, Pena J, Genis D, Rubio F, Peres-Serra J, Barraquer-Bordas L. Balint's syndrome. Report of four cases with watershed parieto-occipital lesions from vertebrobasilar ischemia or systemic hypotension. Acta Neurol Belg. 1982; 82:270–280.
30. Gottfried JA, Mayer SA, Shungu DC, Chang Y, Duyn JH. Delayed posthypoxic demyelination. Association with arylsulfatase A deficiency and lactic acidosis on proton MR spectroscopy. Neurology. 1997; 49:1400–1404.
31. Custodio CM, Basford JR. Delayed postanoxic encephalopathy: a case report and literature review. Arch Phys Med Rehabil. 2004; 85:502–505.
32. Khot S, Walker M, Lacy JM, Oakes P, Longstreth WT Jr. An unsuccessful trial of immunomodulatory therapy in delayed posthypoxic demyelination. Neurocrit Care. 2007; 7:253–256.
33. Thacker AK, Asthana AB, Sarkari NB. Delayed post-anoxic encephalopathy. Postgrad Med J. 1995; 71:373–374.
 XML Download
XML Download