

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dentistry is the health science that includes the study of basic principles and application of these principles to prevent deterioration of the oral structures and the use of pertinent clinical procedures to improve the oral health.1 Frequently patients exposed to fixed restorative procedures experience discomfort in the prepared teeth either during the treatment and sometimes following placement of restoration, which they perceived in the form of pain or other unyielding symptoms, which may be due to dentin hypersensitivity.
Dentin hypersensitivity has been defined as short, sharp pain arising from exposed dentin typically in response to chemical, evaporative, thermal, tactile or osmotic stimuli, which cannot be ascribed to any other form of dental defect or pathology.2 Earlier investigators stated that dentin hypersensitivity is an enigma being frequently encountered, yet ill understood.3
It is reported that approximately 1 to 2 million dentinal tubules are exposed during an average tooth preparation for receiving a posterior crown.4 There has been an extensive use of desensitizing agents over the past few decades due to introduction of newer agents and increased incidence of post-cementation sensitivity.
The restorations luted with cements like zinc phosphate and glass ionomer result in partial removal of the smear layer owing to their acidic nature.5 The cement can displace an equal amount of dentinal fluid, which may cause excessive hydrostatic pressure leading to post-cementation sensitivity. The orifices of the exposed tubules can be sealed off with polymerizable products like dentin bonding agents or with non-polymerizable formulations, which do not require light activation.
The geometric form of the prepared tooth and the casting mainly determines the retention of the prosthesis, but the clinical success of the restoration also depends on the integrity and the mode of attachment of the intervening cement layer.6 The various cementing media ranging from the traditional ones like zinc phosphate cement to the newer resin-based luting cements have different modes of attachment to the casting and the tooth surface.
A myriad of combinations of desensitizers and luting cements are available today to the dental clinician. The available literature offers inconsistent statistics on the effect when using various desensitizing agents with luting cements like zinc phosphate, glass ionomer and resin-modified glass ionomer.
The purpose of this study was to evaluate the effect of two commercially available desensitizing agents, GC tooth Mousse and GLUMA® Desensitizer, on the retentive ability of three luting agents namely zinc phosphate, glass ionomer and resin modified glass ionomer cement when used as luting agent for complete cast crowns.
MATERIALS AND METHODS
Ninety freshly extracted human molar teeth were selected because of their relatively large surface area to resist fracture and their diverging roots to resist removal from the acrylic resin during testing. These molar teeth were obtained from oral surgery clinic and stored in 0.05% sodium azide (Fisher Scientific, Fair Lawn, NJ, USA) to prevent microbial growth.
The selected molar teeth were cleaned with periodontal scalers under tap water to remove any surface deposits and then stored in distilled water at room temperature, with 0.1% thymol as preservative. Notches were made on the root surface with a diamond point to permit better mechanical locking of teeth in acrylic resin. A permanent mark was made on the tooth root, 1 mm below the cementoenamel junction to allow embedding of the specimen upto this level in acrylic resin.
A metal mold with internal dimensions of 25 mm × 19 mm was used for embedding of teeth specimens. The molds were partially filled with autopolymerizing acrylic resin (RR powder & liquid, self-cure acrylic repair material; Dentsply, India) and was allowed to set. The plane of the surveying table was made parallel to the survey platform and checked by using glass slab. Small amount of cyanoacrylate (Fevi Kwik; Pidilite Ind. Ltd., India) was used to position the tooth in its most vertical alignment to the analyzing rod of the surveyor. The mold position was adjusted such that the tooth would be embedded in its center (Fig. 1).
The vertical arm was then lowered till the mark on the root surface was in level with the upper rim of the metal mold. The rings were then filled with autopolymerizing acrylic resin to secure the roots of the extracted teeth. After the resin was polymerized, the analyzing rod was manually separated from the tooth surface. The specimens were stored in distilled water except during tooth preparation, impression making, cementation and testing procedures.
Uniform taper was obtained by the design of a clamp (Fig. 2), which was able to secure a high-speed air-rotor hand piece (NSK, Nakanishi Dental Mfg. Co. Ltd., Japan) to a dental surveyor (Jelenko, J.F. Jelenko & Co., Inc., NY, USA). This clamp maintained the hand piece in a constant relationship with the surveyor. The adjustable vertical arm of the surveyor could change its vertical position. The clamped hand piece could maintain the diamond point absolutely vertical in the coronal and the sagittal plane.
A metal jig was prepared for holding the specimens at the time of tooth preparation. Constant taper of 6 degrees for the preparations was obtained as a negative image of a long round ended tapered diamond point. A wheel shaped diamond point (WR- 13C; Dia-Burs, Mani Inc. Tochigi, Japan) was used to prepare the occlusal surface to the molar teeth, to the depth of the central groove.
Again the constant relation of the firmly clamped handpiece ensured a perfectly flat occlusal surface, parallel to the floor. Axial reduction was achieved by using the long round ended tapered diamond point (TR-26; Dia-Burs, Mani Inc, Tochigi, Japan). A constant length of 4 mm was achieved by marking the desired level on the head of the diamond point and then orienting the mark with the flat prepared occlusal surface. The handpiece was secured vertically at this level by tightening the screw on the vertical arm of surveyor.
The surveying table was then moved on the surveying platform with the handpiece operating simultaneously so as to prepare the axial surface. The stability of headpiece and convergence of the diamond instrument automatically ensured a constant taper of 6 degrees no matter in which direction the surveying table was moved.
A 0.5 mm chamfer gingival finish line, corresponding to half the diameter of the diamond point at its tip was prepared above the cementoenamel junction while maintaining a constant preparation height of 4 mm.
The preparations were finished by using fine grit round ended tapered diamond point (TF-13EF; Dia-Burs, Mani Inc, Tochigi, Japan). The line angles of all the prepared teeth were rounded with abrasive strips.
Thus, all the prepared specimens had a standardized constant total occlusal convergence and a constant height of 4 mm but with variable resultant size of individual tooth. Before the application of desensitizing agents and cementation, the axial surface area of each prepared tooth was determined. The surface area of the preparation was measured by adapting a lead foil closely along the axial surface of the prepared teeth cut where the end overlapped and the length of the foil is measured.
Preparations were then categorized according to the descending order of their surface area and were divided into three groups and each group was further divided into three subgroups. For the ease of understanding, the test samples were Group I zinc phosphate cement (Harvard cement Quick setting, Harvard Dental International GmbH, Hoppegarten, Germany) and Group II glass ionomer cement (GC Fuji I; GC Corporation, Tokyo, Japan) and Group III resin modified glass ionomer cement (RelyX™ Luting, 3M ESPE, MN, USA). The subgroups were divided as C, T and G for Control, GC Tooth Mousse and GLUMA® desensitizer respectively.
Preformed plastic rings of 30 mm × 25 mm size were used as a special tray. Impressions of the prepared teeth were made in polyvinyl silicone impression material (Flexitime, Easy putty and correct wash; Heraeus Kulzer, Hanau, Germany) using the plastic molds. Debubblizer (Debubblizer spray; Prime Dental Products, Mumbai, India) was sprayed on the impression surface to reduce the surface tension and to increase the wettability. The impressions were poured in Type IV die stone (Kalrock; Kalabhai Karson Pvt. Ltd., Vikroli (W), Mumbai, India). The dies were recovered after one hour.
Three layers of die spacer provide a space of 35 - 40 µm.7 Zinc phosphate, glass ionomer and resin modified glass ionomer cement provide a film thickness of 25 µm or less when used in luting consistency. Hence, two layers of die spacer (Color Spacer; Heart-man dental lab., Korea) was applied on the dies, 1 mm short of the gingival finish line to provide space for the luting cement and to allow better marginal adaptation of the castings.
Die hardener (Stone-Die & Plaster Hardener Resin; Heart-man dental Lab., Korea) was applied on the finish line area to prevent abrasion by waxing instruments during the fabrication of the wax pattern. Die lubricant (Die release; Prime Dental Products, Mumbai, India) was applied above the cementoenamel junction. Wax patterns with flat occlusal surfaces were made on dies with Type II casting wax (S-U-Underlay & S-U-Modelling wax, Schuler, Ulm, Germany).
The margins were adapted and excess removed with PKT carving instruments under magnifying glass. The thickness of the wax coping was maintained at 0.5 mm measured with wax gauge (S-U-Iwanson-Feeler Tweezer II for metal; Schular-Dental, Ulm, Germany). A loop was then attached onto the occlusal surfaces of the patterns (Fig. 3). This loop in the cast metal crown would facilitate the engagement of the jig for the retention testing on the universal testing machine.
The wax patterns and dies were assigned numbers corresponding to those on the metal molds of the specimen in order to orient the individual casting on the prepared teeth and prevent confusion. Ten wax patterns were attached to one base former taking care that none of them were contacting each other and a debubblizer solution was applied. Then the patterns were invested in high strength phosphate bonded investment (Wirovest; Bego Corp., Hanau-Wolfgang, Germany).
Wax burnout was carried out in a micro process controlled furnace (AX-4-10B Intellective Burnout Furnace, Tianjin, P.R., China) with the programmed cycle selected for nickel-chromium alloy (Sankin CB-80; Nickel-Chromium for crown and bridge, Dentsply, Delhi, India). Casting was done in a centrifugal casting machine (Unident instruments Pvt Ltd, New Delhi, India). Following casting, the ring was disinvested and the sprues were cut (Fig. 4).
The castings were then gently tried on the dies using the number scribed on them. Marginal adaptation and completeness of seating of the crowns were evaluated. Any casting with either short margins or having an unsatisfactory seat were rejected and newer specimens were prepared in similar manner to replace them. The castings were finished with metal finishing stones and burs followed by sandblasting with 50 µm aluminum oxide particles in the sandblaster (AX-B5; Twin-Pen sandblaster, Titanjin Aixin medical equipment co. Ltd., Tianjin, China). The castings were checked for a good fit on the prepared crowns and thereafter cleaned in an ultrasonic bath (Transonic 470/H, Elma, Singen, Germany) for 60 seconds.
Prior to final cementation the prepared tooth surfaces were treated with two commercially available desensitizing agents (Fig. 5) namely GC Tooth Mousse (GC International, Itabashi-ku, Tokyo, Japan) and GLUMA® desensitizer (Heraeus Kulzer, Hanau, Germany).
A generous layer of GC Tooth Mousse was applied on the prepared tooth surfaces using an applicator tip and left it undisturbed for a minimum of 3 minutes. The smallest possible amount of GLUMA® desensitizer was applied on the prepared tooth surfaces using cotton pellets for 30 - 60 seconds. Then a stream of compressed air was applied until the fluid film has disappeared and the surface was no longer shiny and rinse thoroughly with water. Thirty samples serving as control were left untreated.
In order to achieve a constant film thickness of the cements used for luting the crowns, it was imperative to mix the cements according to manufactures instructions and also to maintain a constant seating force during cementation. The crowns that were lined with cement were initially seated with strong finger pressure. Thereafter, the assembled teeth and crown were placed on the customized jig attached to lower part of the universal testing machine and a static axial load of 5 kg. for 10 minutes was applied.8 The excess cement was removed after setting using an explorer. After completion of the cementation procedures, all the samples were stored at 37℃ for 24 hours before retention test. The retention test of all the samples was performed on the automated universal testing machine (Model 4467; Instron, UK).
A self-alignment jig, mounted on the universal testing machine was used for removal of crowns. The specimens with cemented crowns were secured on the lower part and the upper vertical shaft was lowered until a pin passed through the loop of the crown (Fig. 6). Thus, as the load cells moved apart at the designated crosshead speeds, a perfectly vertical tensional force was applied on the crown and the tooth.
The cross-head speed of the calibrated load cell was set at 0.5 mm/minute as per the recommendations of ADA specification for testing cements.9
The computer connected to the universal testing machine automatically recorded the loads and stressed induced during testing. The number of the specimens was tabulated and the readings obtained after testing were entered corresponding to the specimen tested. The data was organized and prepared for statistical analysis.
Once the crowns had separated from the prepared teeth, the debonded surface was examined carefully to evaluate the mode of failure of the cement under magnification. The failure modes were categorized as follows:10
The failure mode of each group for the three cements was recorded.
Statistical analysis was done by calculating the mean and standard deviation of the subgroups of various groups. The data for dislodgment stress were subjected to one-way analysis of variance (ANOVA) (GraphPad Prism 5.04, GraphPad Software Inc., San Diego, CA, USA) followed by Turkey-Kramer post hoc test. The level of statistical significance was preset at alpha of 0.05.
RESULTS
The one-way ANOVA indicated a significant influence of both desensitizer type (P=.001), cementing agents (P=.001) and their interaction term (P=.001) on crown retentive strength. Debonded stress values were grouped according to types of cementing agent used. The mean, standard deviation (SD) values and results of ANOVA test presented in Table 1 revealed that there was a statistically significant difference between different interactions.
Turkey's post hoc test showed that in Group III (resin modified glass ionomer cement) subgroup G (GLUMA® desensitizer) showed the highest mean of retention, which was statistically significant, followed by subgroup C (Control) and subgroup T (Tooth mousse) which showed the lowest mean retention values. Glass ionomer cement (Group II) demonstrated retentive values between resin modified glass ionomer cement and zinc phosphate cement group. For zinc phosphate cement (Group I), there was no statistically significant difference between subgroup C (Control) and subgroup G (GLUMA® desensitizer) but subgroup T (Tooth mousse) showed the lowest mean retention, which was statistically significant. Fig. 7 shows the categorization of mode of failure of three luting cements. For zinc phosphate cement failure was of adhesive type with cement mainly present on castings. For glass ionomer cement again the failure was of adhesive type but the cement predominantly present on tooth surface. For resin modified glass ionomer cement failure was of adhesive type with cement present on both tooth surface and castings. During testing there was no fracture of casting.
DISCUSSION
Tooth hypersensitivity is one of the oldest recorded complaints of discomfort to people. The use of desensitizing agents following tooth preparation has been increased because of the increase in the reported incidence of post-cementation sensitivity.
Kern et al.11 evaluated the post-cementation sensitivity with zinc phosphate and glass ionomer cements and found it to be similar. The retentive strength of crowns cemented to dentin depends on the physico-chemical properties of the luting agent used. The desensitizing agents applied on the tooth surface can, however, alter the retentive properties of the cementing medium, which is the primary function of luting agent.
This study was intended to evaluate the effect of two commercially available desensitizing agents on the retention of complete cast crowns when cemented with three different luting agents. The reason for the choice of zinc phosphate, glass ionomer and resin modified glass ionomer cements was that post-cementation hypersensitivity is a common complaint with the use of these cements.12
After treating the samples with desensitizing agents as per manufacturer's instructions, complete cast crowns were cemented and were tested on Automated universal testing machine.
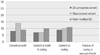
In this study, the mean retentive force required to dislodge the crowns cemented on untreated specimen with zinc phosphate cement, glass ionomer cement and resin modified glass ionomer cement were 27.67 ± 3.39 kg, 39.09 ± 2.80 kg, 48.61 ± 3.54 kg, respectively.
For GC Tooth mousse applied specimen the mean retentive force required to dislodge crowns cemented with zinc phosphate cement was 25.27 ± 4.60 kg, which was found to be reduced when compared with mean retentive force of the crowns cemented with zinc phosphate cement on untreated specimen. This finding confirms with Yim et al.8 who on the basis of their results proved that the bond strength of the luting agents relying on mechanical interlocking into surface irregularities would decrease in bond strength as a result of dentin treatment with a desensitizer. For zinc phosphate cement, any type of dentin desensitizer significantly reduced crown retention to low level.
When on GC Tooth mousse applied specimen, crowns were cemented with glass ionomer cement and resin modified glass ionomer cement the mean retentive force required to dislodge the crowns were 40.32 ± 3.89 kg and 48.34 ± 2.94 kg, respectively. These results were comparable with mean retentive force required to dislodge the crowns cemented with glass ionomer cement and resin modified glass ionomer cement on untreated specimen. This confirms with the conclusion of Mazzaoui et al.13 who stated that when the CPP-ACP complex is added to glass ionomer cement, it increases the bonding strength of the cement by 33 percent. Due to release of minerals such as calcium, phosphate and fluoride ions glass ionomer cement was able to protect the dentin adjacent to the filling.
The possible explanation of these results could be GC Tooth Mousse, when applied on tooth surfaces, fills and smoothes the surface irregularities. Burwell14 in his SEM study found that there were more partially occluded tubules visible on the GC Tooth Mousse-treated samples than the control samples. Zinc phosphate cement, mainly relies on mechanical interlocking into surface irregularities and showed decreased tensile bond strength. Glass ionomer and resin modified glass ionomer cement bond both mechanically and chemically and thus application of GC Tooth Mousse does not reduce the retentive force when compared with control.
When GLUMA® Desensitizer was applied as a desensitizing agent on the prepared tooth surfaces the mean retentive force required to dislodge the crowns when cemented with zinc phosphate cement is 27.92 ± 3.20 kg, glass ionomer cement is 41.14 ± 2.42 kg and resin modified glass ionomer cement is 49.02 ± 3.32 kg. These findings were comparable with control subgroups of all three cements. This result is in consistent with Swift et al.15 who stated that GLUMA® desensitizer do not reduce the retention of cast metal crowns luted with a zinc phosphate, conventional glass ionomer or resin modified glass ionomer cement. Johnson et al.16 in their study concluded that GLUMA® desensitizer was used in combination with the zinc phosphate, glass ionomer and modified glass ionomer cement without affecting the retentiveness of castings.
The possible justification could be GLUMA® desensitizer, a non-polymerizable resin sealer precipitates within the tubules when applied onto prepared tooth surfaces. Arrais et al.17 in their SEM analysis stated that tooth surface when treated with GLUMA® desensitizer obliterates majority of dentinal tubules and infiltrates into tubules as plugs. Thus, GLUMA® desensitizer does not affects the dentin surface irregularities that aid in mechanical retention for zinc phosphate and hence the casting retention was unaffected when compared with control samples. The acid polymers of the glass ionomer and resin modified glass ionomer cement may have a chemical affinity to the resin sealer, which contains glutraldehyde and hydroxyethyl methacrylate monomers.
The failure modes of the cement also reflect these characteristics. For zinc phosphate cement the failure was of adhesive type with most of the cement present on the castings. For glass ionomer cement showed adhesive failure with cement predominantly present on the prepared tooth surface. Resin modified glass ionomer cement showed adhesive type of failure with cement present on both prepared tooth surface and castings.
Clinicians perform crown and bridge restorative procedures on a regular basis. Desensitizing agents should be used routinely on all abutment teeth to be restored with fixed restorations not only to prevent dentin hypersensitivity but equally important to minimize bacterial contamination to reach the pulp. The desensitizing agents GC Tooth Mousse and GLUMA® desensitizer can be accepted as blanket treatment in crown and bridge prosthodontics.
Hence, judicious use of GC Tooth Mousse and GLUMA® desensitizer is advisable in routine clinical practice for prosthodontists and general practitioners for reducing complaint of post-cementation hypersensitivity.
CONCLUSION
Application of desensitising agents like GC Tooth Mousse and GLUMA® desensitizer may be indicated during fabrication of simple or complex fixed partial dentures as it will not affect the retentive ability of the luting cements. An in vivo study may be required to prove its effect, thereby utilizing this therapy as blanket treatment to the denuded dentin surfaces and thus can be turned as a boon to the patient at large.
Within the limitations of the study, we can conclude that:
GLUMA® desensitizer as desensitizing agent improves the retention of cast crowns when used with zinc phosphate, glass ionomer and resin modified glass ionomer cement.
GC Tooth Mousse when applied on prepared tooth surfaces caused increase in retention of cast crowns prior to cementation with glass ionomer and resin modified glass ionomer cement.
GC Tooth Mousse when used prior to cementation of cast crowns with zinc phosphate cement did reduce the retentive strength of the cement.







 XML Download
XML Download