

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Asthma management guidelines recommend anti-inflammatory controller therapy to attenuate chronic airway inflammation in persistent asthma.123 Inhaled corticosteroids (ICSs) are available inpressurized metered dose inhalers (pMDI) using a hydrofluoroalkane propellant as both fine-particle formulations with a particle mass median aerodynamic diameter (MMAD) of 2-4 µm and as aerosols of extrafine particles with an MMAD-1 µm.456
Ciclesonide is an extrafine-particle ICS (MMAD 1.0 µm) that shows both high lung deposition and peripheral lung distribution in healthy volunteers and patients with asthma.78 Results of small studies in patients with mild-to-moderate asthma indicate that ciclesonide improves inflammation and patency of small airways9 and, compared to fluticasone (MMAD 2.4-2.6 µm), provides greater improvement in small airway function, inflammation, and hyperresponsiveness to small-particle aerosolized adenosine monophosphate (MMAD 1.04 µm).1011 As small airways dysfunction may be involved in unstable asthma, 4121314 these findings raise the question whether there are differences ineffectiveness between extrafine- and fine-particle ICSs.
In clinical trials to date, ciclesonide showed similar efficacy as compared with fine-particle ICSs, such as fluticasone and budesonide (MMAD ~3 µm) at similar nominal doses for patients with persistent asthma.101516 However, these trials were generally 8-12 weeks in duration and focused on short-term improvement of lung function outcomes, thus they were unable to assess longer term fluctuations in asthma control and events, such as exacerbations. Moreover, smokers and patients with unstable asthma, who may both have more prominent small airways disease,417 were typically excluded, as were patients with poor inhaler techniques, who might also benefit from extrafine-particle ICSs.18 Thus, the question remains whether ICS particle size plays a role in long-term effectiveness of ICS therapy.
Non-interventional observational studies using high-quality databases can capture prescribing and medical record information to assess long-term outcomes for patients with asthma often excluded from clinical trials but commonly seen by clinicians, such as smokers, patients with poor inhaler techniques, patients at high risk of exacerbation, and those with comorbidities. 14171920 Previous database studies in the UK and USA have found in matched cohort analyses that the prescription of extrafine-particle beclomethasone was associated with equal, or better, asthma-related outcomes over a 1-year period, at significantly lower prescribed ICS doses, than standard fine-particle fluticasone.2122 The aim of the current historical cohort study was to compare 1-year asthma-related outcomes between extrafine particle ciclesonide and 2 standard fine-particle ICS, fluticasone and non-extrafine beclomethasone, for patients in the Netherlands prescribed their first ICS.
MATERIALS AND METHODS
Data source
This was a historical, matched cohort effectiveness study of patients registered from September 2005 through December 2012 in the PHARMO Database Network (PHARMO Institute, Utrecht, The Netherlands), which links outpatient pharmacy and hospital discharge records for a catchment area representing 3.6 million residents (additional detail is provided in the Online Supplement).232425 The study was conducted to standards suggested for observational research, including an independent advisory group, use of an a priori analysis plan, and study registration.262728
Patients and study design
Patients eligible for this study were aged 12-60 years, had ≥1 full year of baseline and ≥1 full year of outcome data before and after their first recorded prescription of ICS (initiation date), and had received 2 or more prescriptions for asthma at any time in their records in addition to the first ICS prescription, including at least 1 more ICS prescription during outcome (but no ICS during the baseline year); therefore, all patients included received at least 2 ICS prescriptions. We excluded patients >60 years old, those with any other recorded chronic respiratory disease, and those prescribed long-acting muscarinic antagonists or maintenance oral corticosteroid therapy during the baseline year.
At the initiation date, patients received a first prescription of ICS delivered using a pMDI as the extrafine-particle ICS ciclesonide (Alvesco®, Takeda Pharmaceuticals International GmbH, Zurich, Switzerland) or a pMDI fine-particle ICS, either fluticasone propionate (Flixotide®, GlaxoSmithKline, Brentford, Middlesex, UK) or non-extrafine beclomethasone dipropionate (Supplementary Fig. 1).
Study endpoints
Co-primary endpoints were assessed during 1 outcome year after initiation of ICS therapy and included (1) the rate of severe exacerbations, defined as asthma-related hospital admission or acute oral corticosteroid prescription (based on the American Thoracic Society/European Respiratory Society definition29 excluding emergency department attendance, not available in the database); (2) risk-domain asthma control, defined as the absence of severe exacerbations; and (3) overall asthma control, defined as achieving risk-domain asthma control plus mean daily dose of albuterol of ≤200 µg. Secondary endpoints included the change in therapy and mean daily dose of short-acting β2-agonists (SABA) during the outcome period (additional detail in the Online Supplement).
Statistical analysis
Analyses were carried out using IBM SPSS Statistics version 22, Microsoft Office EXCEL 2007, and SAS version 9.3. Statistical significance was defined as P<0.05. Chi-square or Mann Whitney U-tests (unmatched data) and conditional logistic regression (matched data) were used to compare treatment cohorts at baseline.
Patients in the 2 cohorts were matched using 1:1 exact-matching methods,30 described in the Online Supplement. Matching variables were sex, age, baseline risk-domain asthma control, prescribed long-acting β2-agonist, SABA daily dose, prescribed leukotriene receptor antagonist, prescribed antifungal medication for oral candidiasis, and year of ICS therapy initiation.
A conditional Poisson regression model was used to compare the rates of severe exacerbations and hospitalizations for matched patients. Conditional binary logistic regression was used to compare the odds of achieving asthma control, being prescribed higher doses of SABA, and changing therapy. Rate ratios and odds ratios, with 95% confidence intervals, were adjusted
for appropriate non-collinear confounders.
RESULTS
Patients
There were 4,064 eligible patients identified in the database during the study period; 1,382 (34%) were prescribed extrafine-particle ciclesonide, and 2,682 (66%) fine-particle ICS. Applying the matching criteria led to 1,244 patients being selected in each treatment cohort (Supplementary Fig. 2).
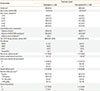
After matching, baseline asthma control measures, SABA daily dose, and prior maintenance asthma therapy were comparable between the cohorts (Table 1). Asthma-related hospital admissions during the baseline year, while generally infrequent, were significantly more prevalent in the ciclesonide cohort (Table 1); significantly more patients who received ciclesonide had evidence of rhinitis (43% vs 38%; P=0.004) and were prescribed proton pump inhibitors (41% vs 34%; P<0.001) than those who received fine-particle ICS.
At the initiation date, ciclesonide was prescribed at significantly lower doses than fine-particle ICS (median [interquartile range] 160 [160-160] vs 500 [250-500] µg; P<0.001). The distribution of doses at initiation (Fig. 1) shows clear separation between ciclesonide (mostly 160 µg/day) and fine-particle ICS (mostly ≥500 µg/day, especially for fluticasone) (Supplementary Table 1).
Co-primary endpoints
During the outcome year, patients prescribed ciclesonide had significantly lower severe asthma exacerbation rates (adjusted rate ratio [95% CI], 0.69 [0.53-0.89]) and significantly greater odds of achieving risk-domain asthma control (defined as absence of asthma-related hospital admissions and of prescriptions of acute oral corticosteroids) and overall asthma control (defined as risk-domain asthma control plus average daily dose of ≤200 µg albuterol) than those receiving fine-particle ICS therapy, after adjusting for baseline confounders (Table 2 and Fig. 2).
Secondary endpoints and other outcomes
Patients in the ciclesonide cohort received fewer prescriptions of other respiratory drugs and had significantly lower ICS daily dose exposure than the fine-particle ICS cohort during the outcome year (Table 3). The odds of a change in therapy during the outcome year were significantly lower for patients prescribed ciclesonide than those prescribed fine-particle ICS (adjusted odds ratio [95% confidence interval], 0.70 [0.59-0.83]). Similarly, the odds of being prescribed a higher SABA dose during the outcome period significantly favored the ciclesonide cohort (Table 2 and Fig. 2). Subanalysis results for the patients with evidence of rhinitis (prescribed nasal corticosteroids) were similar to those of the main analysis (Supplementary Table 2).
During the outcome year, patients prescribed ciclesonide received a significantly higher ratio of controller-to-total medication than those prescribed fine-particle ICS (Table 2). Although patients in the ciclesonide cohort had higher hospital admissions during the baseline year compared with those receiving fine-particle ICS (1.9% vs 0.5%; P=0.002), this difference was no longer observed during the outcome year after ICS initiation (0.7% vs 0.6% patients prescribed fine-particle ICS; P=0.81; Table 2).
Prescriptions of oral antifungal medications for treating oral candidiasis were similar in both treatment cohorts at baseline and during the outcome year.
DISCUSSION
In our population-based matched cohort study, we observed that patients prescribed extrafine-particle ciclesonide experienced significantly lower rates of severe exacerbations, i.e., hospitalizations or acute oral corticosteroid courses, in the first year after initiating ICS treatment than those prescribed fine-particle ICS, and ciclesonide prescribing was associated with better odds of achieving asthma control. Patients prescribed ciclesonide were also significantly less likely to require a change in therapy or higher doses of reliever medication than those prescribed fine-particle ICS. Notably, the prescribed doses of ciclesonide were one-third those of fine-particle ICS at the initiation date despite matching for patient characteristics (median dose, 160 vs 500 µg/day); and ICS dose exposure during the outcome year was also significantly lower for the ciclesonide cohort (median, 126 vs 332 µg/day). The drop in the dose of both ICS from the initial prescribed dose was likely the result of incomplete adherence during the outcome year, a common finding in real life.31
We matched the cohorts for important clinical asthma parameters, including baseline risk-domain asthma control status (capturing asthma-related hospitalizations and oral corticosteroid bursts during the baseline year), baseline SABA dose, and demographic characteristics (sex and age). Nevertheless, the ciclesonide cohort presented with signs of more difficult-to-control asthma at baseline in the form of greater frequency of nasal corticosteroid and proton pump inhibitor prescriptions.132 This would presumably favor better asthma control in the outcome year for the fine-particle ICS cohort. Moreover, despite higher baseline hospital admissions in the ciclesonide than in the fine-particle ICS cohort, there was no difference in outcome hospitalizations. These findings suggest a clinically significant improvement in asthma control for patients prescribed ciclesonide who had unstable disease and thus would classically be excluded from randomized controlled trials.
Possible mechanisms to explain better effectiveness of ciclesonide include (1) improved airway drug distribution, including small airways;47810 (2) decreased impact of errors in inhalation techniques (especially poor coordination or too fast inhalation flow rate) on lung deposition;3334 and (3) improved adherence, promoted by greater perception of treatment effects, once daily dosing, or reassurance as to the dose of corticosteroid. Moreover, compared to those prescribed fine-particle ICS, more patients prescribed ciclesonide had a controller-to-total medication ratio of ≥0.5, a finding associated with improved asthma-related quality of life, better disease control, and reduced symptoms.35
There are several limitations to this study. Exclusion of patients without data during a 1-year period before and 1 year after ICS initiation meant that patients who moved or died were not represented. The requirement that all patients have 1-year outcome data predisposed the study to survivor bias. However, this may not have had a major effect, given the median age of 45 years and because patients prescribed their first ICS are unlikely to have severe asthma. Other limitations are those common to observational studies: biases deriving from unmeasured confounders that may particularly affect 1 of the 2 treatment strategies, non-random assignment of drug treatment, and potential misclassification bias and under-reporting if medical attention was not sought.
During the study period, ciclesonide was not the most common ICS prescribed in the Netherlands, although it was prescribed for 34% of patients. Thus, there may be unrecorded reasons physicians chose to prescribe ciclesonide, resulting in prescription bias. This channeling phenomenon was suggested given that patients prescribed ciclesonide had signs of difficult-to-treat asthma (rhinitis and gastroesophageal reflux),32 find-ings potentially reducing positive effects of ciclesonide versus fine-particle ICS on asthma outcomes, which was not the case. While 1,244/1,382 (90%) eligible patients initiating ciclesonide were matched, only 1,244/2,682 (46%) of those initiating fine-particle ICS were matched, suggesting the possibility that patients in the fine-particle cohort were not representative of those who initiate fine-particle ICS therapy in the Netherlands.
Finally, our analyses were limited by data availability; for example, smoking history, which may have some impact on effectiveness of ICS,1736 was not available, and nor were body mass index and lung function data. Diagnostic information was inferred from prescribing data. This meant that patients were selected as having asthma based on prescribed therapy, potentially leading to diagnostic misclassification. To mitigate this, we excluded patients with only 1 ICS prescription, which could have been a therapy trial. We were not able to assess current clinical control, but SABA dose (based on prescriptions) served as an indication of symptom control: 83% and 64% of patients in the ciclesonide and fine-particle ICS cohorts, respectively, were prescribed ≤1 puff/day (≤100 µg/day) of SABA on average, well within the definition of good control of asthma from an administrative database.37 The actual use of SABA was likely lower, as patients tend to have multiple inhalers and do not use all of the prescribed canisters.
This study also has several strengths. Patients were drawn from a large diverse population with subsequent 1:1 exact matching on key baseline characteristics to ensure that the 2 cohorts were as comparable as possible with respect to demographic and clinical characteristics.30 Outcome measures were adjusted for appropriate non-collinear baseline confounders. The 1-year baseline and outcome periods enabled us to identify measurable changes in endpoints, such as hospitalizations, severe exacerbations, and asthma control, and also to allow for seasonal changes in respiratory conditions. All patients were prescribed the same inhaler type for ICS (pMDI), minimizing outcome differences associated with inhalation techniques for ICS or mixing inhaler devices (most SABA inhalers prescribed in the Netherlands are pMDIs).638
The residual baseline differences between treatment cohorts after matching (i.e., greater frequency of rhinitis and gastroesophageal reflux prescriptions in the ciclesonide treatment cohort) were addressed in the statistical models. Nasal corticosteroid prescriptions were not significant in the statistical model for the co-primary endpoints, suggesting that these did not affect the results, and the subgroup analysis of patients receiving nasal corticosteroid prescriptions corroborated the main findings. The co-primary endpoints were all adjusted for proton pump inhibitor prescriptions.
Guidelines recommend that fluticasone and ciclesonide be prescribed at similar nominal doses123615 based on equipotence in formal testing in randomized trials. Despite these recommendations, we found that in practice, ciclesonide was prescribed at lower doses than fluticasone and that fluticasone was typically prescribed at higher than recommended doses, corroborating findings from prior studies in the Netherlands, as well as New Zealand, the UK, and the USA.21223940 Lower doses of ICS may be associated with reduced adverse events;4142 further research is required to determine whether the lower prescribed doses of ciclesonide and of extrafine-particle beclomethasone in prior studies2122 are associated with fewer adverse events in real-life populations, an important consideration for long-term asthma controller therapies and one that requires further studies, as we could not capture drug-related adverse events from our data source. Extrafine-particle ICS have relatively low oropharyngeal deposition, which could potentially lead to fewer oral side effects than with larger particle ICS.8151843 However, we found that the proportion of patients prescribed antifungal medication for oral candidiasis was low and similar in the ciclesonide and fine-particle ICS treatment cohorts (2.3% vs 1.5%).
In conclusion, the results of this matched cohort analysis suggest that initiation of ICS with ciclesonide is associated with better 1-year asthma outcomes and fewer changes to therapy in that year, at one-third of the prescribed dose than with fine-particle ICS. The study drew on reliable dispensing and hospitalization data for a real-life Dutch population—presumably including smokers and non-smokers, patients with good and bad inhaler techniques, stable and unstable asthma, and good and bad adherence. The association of better outcomes with cicle-sonide therapy was present, even though asthma was somewhat more severe in those prescribed ciclesonide. More real-life observational or randomized controlled studies of other patient populations and different extrafine-particle ICS are needed to further explore these findings.




 XML Download
XML Download