

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atopic dermatitis (AD) is a chronic, pruritic inflammatory skin disease and is one of the most common allergic diseases in children. The prevalence of AD is currently increasing and the incidence in children is reported to range from 15%-30% worldwide.1,2 Although the occurrence of AD is associated with genetic factors,3,4 recent rising incidence rate is more likely to be related with environmental factors.5,6,7 Many studies have reported on the effects of aeroallergens including pet hair, house dust mite, pollen, and others on the deterioration of AD.8,9,10,11,12 In addition, the role of environmental pollutants on the occurrence and deterioration of AD has been investigated.13,14,15 Airborne particulate matters (PM) have been identified to be one of the risk factors related with deteriorating skin condition of AD patients.16 Indoor redecoration activities before birth and in the first years of life are associated with the development of AD in early childhood.17 Exposure to volatile organic compounds (VOCs) can damage the epidermal barrier and enhance adverse effects of house dust mites on sensitized subjects with AD.18 Exposure to formaldehyde and nitrogen dioxide (NO2) at domestic concentration can cause skin barrier function impairment in patients with AD.15 High levels of Staphylococcus aureus may contribute to disease severity and persistence in AD patients.19
The concentrations of indoor air pollutants are affected by lifestyle and residential environment.20 Identifying sources of indoor air pollution could be beneficial in creating favorable environment for AD patients. However, there was no report on the residential environments in relation to the concentrations of indoor pollutants in Korean houses. This study was aimed to investigate the relationship between residential environment and indoor air pollutant levels in the houses of AD patients living in Seoul, Korea.
MATERIALS AND METHODS
Participants
The study subjects comprised 150 AD patients living in Seoul. Assessment of residential environment was by a questionnaire and direct measurement of indoor air pollutant levels was conducted in the residences of all the subjects from March, 2008 to April, 2010. The diagnosis of AD was conducted by Hanifin and Rajka's diagnostic criteria.21 This study was approved by the institutional review board at Samsung Medical Center in Seoul (IRB approval number: 2013-02-024-001). Written informed consent was obtained from parents prior to participation in the study.
Assessment of residential environments by questionnaires
The parents of all participants were asked to complete a questionnaire for assessing residential environment. The contents of the questionnaire included age, gender, socioeconomic status (monthly family income, educational background of mother) and environmental factors relating to indoor air quality (parental smoking, frequency of vacuuming and frequency of ventilation, distance to nearest major roads, facilities within 2 km of the home, building type, type of floors, indoor renovations within 5 years, moving to newly constructed house within 1 year, carpet, fabric sofa, air cleaner, air conditioning, humidifier, insecticide use and indoor domestic pets).
Direct measurement of indoor air pollutant concentrations
Indoor air pollutant concentrations were measured including particulate matter with diameter less than 10 µm (PM10), formaldehyde, carbon dioxide (CO2), carbon monoxide (CO), nitrogen dioxide (NO2), total volatile organic compound (TVOC), benzene, toluene, ethyl-benzene, xylene, styrene, bacterial aerosols and airborne fungi.
Mini-volume Air Sampler, Model 4.1 (Airmetrics Co, Eugene, OR, USA) was used to sample PM10. Each sample collection was conducted in the living room for 8 hours during the daytime at a constant sampling flow rate of 10 L/min. The sampling spot was chosen at a place 1 meter or more away from the walls, ceiling and floor, and the sampler was positioned 1.2-1.5 meters above the floor. Formaldehyde was assessed using personal air sampler (SIBATA MP -Σ100H, Japan). Sampling was for 30 minutes at a flow rate of 1 L/min. TVOC was assessed using a stainless steel adsorption tube (1/4 inch×9 cm, PerkinElmer, Inc., Shelton, UK) charged with 200 mg or above Tenax-TA (60/80 mesh; Supelco, Bellerfonte, PA, USA) through solid-phase adsorption. This sampler was also positioned 1.2-1.5 meters above the living room floor and at the same height in a child's room. Sampling was for 30 minutes at a flow rate of 0.1 L/min. A Turbomatrix ATD (PerkinElmer Inc) heat processor, and various types of gas chromatography (GC-MSD, HP-6890 and Agilent 5973; Hewlett-Packard, USA; Agilent, USA) were used in the analyses. The pump used in capturing CO, CO2 and NO2 gases was APEX personal air sampler (Casella, Bedford, UK) with reduced fluctuating flow rate before and after sampling. These gases were consecutively collected in a 10 L tetra bag (Supelco) at a flow rate of 1 L/min, and analyzed by a gas analyzer (Eco-tech, Australia). Bacterial aerosols and airborne fungi were assessed using a model 10-880 Single Stage Ambient Viable Sampler (Tisch Environmental, Cleves, OH, USA). Tryptic Soy Agar (TSA) for bacterial aerosols, Malt Extract Agar (MEA) for airborne fungi was the medium. Microbial sampling lasted for 5 minutes at a flow rate of 28.3 L/min 1.2-1.5 meters above living room and child's room floors. The media were cultivated in a MIR252 incubator (SANYO, Japan) at 35℃ for 48 hours. Colony forming units (CFU) per area was calculated by dividing CFU value by indoor air volume.
Statistical analyses
Data gathered through indoor environment assessment and survey was analyzed using SAS version 9.1 (SAS Institute, Cary, NC, USA). All values are presented as the mean±SD. The correlation between various environmental factors in questionnaires and the direct measurement values of indoor air quality was examined by Pearson correlation analysis to select the residential environment mainly contributing indoor air pollution. Subsequently, influencing variables were adjusted and are presented as least squares mean±standard error. A one-way ANOVA was conducted to compare the relationship between the direct measurement values of indoor air quality and the residential environment mainly contributing indoor air pollution. Influencing variables were adjusted by analysis of covariance (ANCOVA). The results were determined to be statistically significant if the P value was<0.05.
RESULTS
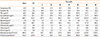
AD patients comprised of 93 boys and 57 girls. The mean age of the respondents was 27.0±21.7 months (range 2-168 months). Table 1 shows the distributions of indoor air pollutants levels. Furthermore, the descriptive statistics are shown for temperature, humidity, PM10, formaldehyde, TVOC, benzene, toluene, ethyl-benzene, xylene, styrene, bacterial aerosols and airborne fungi levels.
The relationship between the residential environment and indoor air pollutant levels are presented in Figure. Pearson correlation analysis was used to examine the relationship between each environmental factor in the questionnaires and the concentrations of each indoor air pollutant. Those factors with no statistical significance were excluded. For the next analysis, we selected the environmental factors with P value<0.05 and 0.05-0.15, although the latter were weakly statistically significant. One-way ANOVA was conducted on the environmental factors with P<0.15.
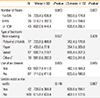
Presence of visible mold on the walls was significantly correlated with concentration of PM10 (P=0.038) (Table 2), while other contributing factors such as construction year, number of floors, indoor renovation and ventilation type were not statistically significant. This difference persisted after adjusting with the other contributing factors (P=0.047).
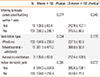
The concentration of formaldehyde was significantly related with the house construction year (P=0.005) and moving to a newly constructed building within 1 year (P=0.005) (Table 3). However, no significant difference was found after adjustment. The concentration of TVOC was significantly high with mixed type of ventilation (P=0.009) and the use of artificial air freshener (P<0.001). When adjusted with age, gender, temperature, humidity, building type, construction year, distance to the nearest major roads, ventilation type, type of heating fuel, indoor domestic pets, type of bedroom floor covering, use of air cleaner and use of artificial air freshener, a significant difference was persistent in TVOC concentrations with the use of artificial air freshener (P=0.003) (Table 4).
We also analyzed the concentration of each air pollutant constituting indoor TVOC, including benzene, toluene, ethyl-benzene, xylene and styrene. The indoor concentration of benzene exhibited significant relationships with ventilation types (P=0.035), and the use of artificial air freshener (P=0.016). After adjustment of confounding factors, a statistical significance was still present concerning ventilation type (P=0.028) and the use of artificial air freshener (P=0.015). A significantly high concentration of benzene was observed in case of 'almost no ventilation' compared with ventilation through windows or a central ventilation system (Table 5). The concentrations of toluene and ethyl-benzene were significantly high with the use of artificial air freshener (P=0.012 and P=0.027, respectively) even after adjustment (data not shown). The concentration of xylene exhibited a significant relationship only with heating fuels (P=0.015). Concentration of xylene was significantly higher when oil was used as fuel than gas or electricity (data not shown). The concentration of styrene was significantly related with building type (P=0.005) after adjustment. Concentration of styrene concentration was significantly higher in a residential and commercial complex building than a detached house, apartment or row house. Although styrene concentration seemed to be related with new furniture or electronics, use of air purifier, use of artificial air freshener and air-purifying indoor plants, there was no significant difference (data not shown).
With regard to bacterial aerosols, a significant difference was shown by the use of air cleaner (P=0.045) when the contributing factors were adjusted. The indoor concentration of bacterial aerosols was significantly low with the use of air cleaner (Table 6). The concentration of airborne fungi had significant relationships with ventilation type (P=0.034) and indoor domestic pets (P=0.001). However, this difference disappeared when adjusting with confounders (Table 7).
When the relationship between CO2 concentrations and residential environment survey was analyzed, the concentration of CO2 was significantly low when moving to a newly constructed building within 1 year (P=0.017). In contrast, CO2 concentration was significantly high for residences containing pets (P=0.003). Although the concentration of CO2 was related with the number of floors and the purchase of new furniture or electronics, no statistical difference was observed (data not shown). The concentration of CO was related with types of living room floor covering, moving to a newly constructed building and the use of artificial air freshener among survey items. However, no significant difference was found after the adjustment (data not shown). The indoor concentration of NO2 showed a significant relationship with ventilation type among effective factors in residential environment survey (P=0.013). A significant difference was also observed after adjusting confounding factors (P=0.028). A significantly high concentration of NO2 was observed in case of 'almost no ventilation' compared with ventilation through windows or a central ventilation system (data not shown).
DISCUSSION
In several studies, indoor air pollution has been considered to act as an aggravating factor in AD.22,23,24 More attention need to be paid to indoor air quality in AD patients, because AD is most prevalent in infants and young children and they spend most of their time indoors. Therefore, it is important to detect hazardous indoor air pollutants to prevent exacerbation of AD symptoms. Although direct measurement of indoor air pollutant level is the best way, it is not easily available in every house of individual AD patient. In this study, we measured the concentrations of 13 indoor air pollutants by visiting the residence of each AD patient and investigated which residential environment could be attributed to increased level of each air pollutant in an attempt to evaluate indoor air quality indirectly. In particular, our results would be helpful for Korean children with AD, because residential environment varies in each region according to life style, economic status and outdoor air pollutant level.
In homes, particles from combustion (e.g., use of wood stoves, kitchen cooking and candles) and tobacco smoking are major components of indoor air pollution.25,26 Higher prenatal exposure to fine particulate matter combined with postnatal exposure to environmental tobacco smoke may increase the risk of infant eczema.27 A moderate increase in long-term exposure to background ambient air pollutants such as ozone and PM10 has been associated with an increased prevalence of AD in children.28 The concentration of ambient ultrafine particles may exacerbate skin symptoms in children with AD.29 Our study showed that significantly high concentration of PM10 was related with visible mold on the walls. As PM includes particles from fungi,30,31 our result suggests that removal of visible mold might be helpful to lower indoor PM10 concentration.
Formaldehyde is a well-known irritant of the upper respiratory tract with symptoms such as eye, nose and throat irritation commonly associated with indoor exposure to the gas. Indoor sources of formaldehyde include particle board, plywood, fireboard, paneling, urea formaldehyde foam insulation and some carpets and furniture, as well as some household chemicals.32 Exposure to low concentrations of formaldehyde for a short period of time influences skin surface parameters, especially the skin barrier function, in patients with AD.15 Low level exposure to indoor formaldehyde may increase the risk of allergic sensitization to common aeroallergens in children.32 In one study, participants experiencing recent indoor renovation showed the odds ratios of 1.9 (95% CI: 1.4-2.7) for eczema.17 As the level of formaldehyde increases in cases of moving to a newly-built building or a renovated house,33,34 lowering formaldehyde level should be taken into account if there is a family member with AD.
Floor wall coverings were the most influential source of indoor VOCs, followed by household cleaning products, wood paneling/furniture, paints and moth repellents.35 Exposure to VOCs can damage the epidermal barrier and enhance adverse effects of house dust mites on sensitized subjects with AD.18 The recruitment and differentiation of eosinophil/basophil progenitors in response to exposure to environmental tobacco smoke (ETS)-related VOCs during pregnancy or at 1 year of age may play a role in the development of AD or cradle cap during the first year of life.36 In this study, the use of artificial air freshener was significantly associated with high concentrations of benzene, toluene, ethyl-benzene and TVOC, supporting previous data.37 Building type was also one of the factors related to indoor air pollutants including styrene. The levels of volatile substances such as styrene were significantly high in commercial buildings. Our results were similar to those from the previous studies where the levels of volatile substances, particulate matter and CO2 were high due to a large transient population and displaced various products in buildings.38 Heating fuel was related to xylene, since the concentration of xylene was significantly high with the use heating oil as the fuel. Xylene is one of the basic and primary oils produced in the petroleum and petrochemical industries. It has been reported to increase the risk of sick house syndrome along with toluene and TVOC.39 The indoor concentrations of CO2 and airborne fungi were significantly high in case of subjects raising domestic pets. When individuals are frequently exposed to domestic pets, they could be infected by fungus such as Stachybotrys chartarum.40,41 With regard to indoor bacterial aerosols, a significantly low concentration was associated with the use of air cleaner.
The aim of this study was not to verify the causality between the indoor air pollution and exacerbation of AD symptoms, but to investigate the relationship between the residential environment and indoor air pollutant levels in the homes of Korean children with AD. In addition, some limitations should be considered when interpreting our results. First, our results did not represent general Korean life style, because the residential areas of the participants in this study were restricted to Seoul, the largest metropolitan city in Korea. Secondly, we measured the concentrations of indoor air pollutants at a single time point in each house, although the questionnaire solicited information on the life style and environmental change in the previous 12 months. The measured levels possibly did not reflect the exact level of exposure to each air pollutant, because those levels might be influenced by various confounding factors on a daily basis.
In conclusion, the residential environment of AD patients living in Seoul is closely related with each indoor air pollutant levels. To alleviate AD symptoms, identifying aggravating factors including indoor air quality is important. In this regard, simple questioning about aspects of residential environment such as visible fungus on the walls and the use of artificial air freshener are helpful to assess the possibility of increased indoor air pollutant levels when direct measurement is not feasible.








 XML Download
XML Download