

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Aspirin-exacerbated respiratory disease (AERD) is characterized by severe and persistent inflammation in the upper and lower airways followed by asthma, nasal polyps, and sensitivity to aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs).1,2 The prevalence of AERD has been estimated as 21% in adults with asthma.3 Although the mechanism of AERD pathogenesis has not been clearly defined, it has been suggested that the disease can be attributed to a significantly higher level of cysteinyl leukotrienes (cys-LTs) compared to aspirin-tolerant asthma (ATA) patients.4 In addition, sarco/endoplasmic reticulum Ca2+ ATPase (SERCA) protein and orosomucoid 1-like 3 (ORMDL3) gene involved in airway remodeling, mediate the endoplasmic reticulum (ER), have provided new insights on bronchial asthma.5,6
ER stress, or ER stress induced apoptosis, caused by accumulation of unfolded or misfolded proteins in the lung epithelial cells is involved in chronic obstructive pulmonary disease.7 Moreover, a new insight into the molecular mechanism connecting Ca2+ signaling-mediated cellular stress in the ER through an ER-resident transmembrane protein ORMDL3 and inflammatory responses suggests that ER stress activates NF-kappaB and may play a role in chronic inflammatory diseases such as asthma.6
The activating transcription factor 6 beta (ATF6B; MIM no. 600984) is an isoform of activation transcription factor 6 (ATF6) that is mainly expressed in the ER. The ATF6B of 110 kDa is cleaved during ER stress and produces a nuclear form of 60 kDa ATF6B.8 Through the repression of ATF6α (the other ATF6 isoform), the ATF6B activates the expression of many ER stress response (ERSR)-related genes such as glucose-regulated protein 78 (GRP78),9 indicating that ATF6B is essential in ATF6α functioning during ERSR.10 More recently, a genome-wide association study has identified a chromosomal region, which includes ATF6B that is associated with lung function such as the ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC).11
Based on the possible relations of ATF6B to asthma and obstructive lung diseases, we hypothesized that ATF6B SNPs might be associated with AERD development and/or the decline of forced expiratory volume by aspirin provocation.
MATERIALS AND METHODS
Study subjects
This study was carried out in compliance with the Global Initiative for Asthma (GINA) Global Strategy for Asthma Management and Prevention Study. Subjects were recruited from the Asthma Genome Research Center comprising the hospitals of Soonchunhyang and Chung-Ang University in Korea. All subjects provided their informed consent, and the study protocols were approved by the Institutional Review Board of each hospital.
All patients in the study had a history of dyspnea and wheezing in the past 12 months, along with one or more of the following: (1) either a ≥ 15% increase in FEV1 or a > 12% increase in FEV1 plus 200 mL follow-up inhalation of a short-acting bronchodilator, (2) <10 mg/mL PC20 methacholine, and (3) ≥20% increase in FEV1 following 2 weeks of treatment with inhaled steroids and long-acting bronchodilators. In addition, 24 common inhalant allergens were used to conduct a skin prick test. Total IgE was measured with the CAP system (Phadia, Uppsala, Sweden), and atopy was defined as having a wheal reaction equal to or greater than the histamine or 3 mm in diameter. An oral aspirin challenge (OAC) was performed with increasing doses,12 based on the updated practice parameter (2010) of the American College of Allergy, Asthma & Immunology/American Academy of Allergy, Asthma & immunology.13,14 Briefly, patients with a history of aspirin hypersensitivity were given 30 mg orally. Respiratory and nasal symptoms, blood pressure, external signs (urticaria and angiooedema), and FEV1 were documented every 30 min for a period of 1.5 h. At the end of this period, if there were no symptoms or signs suggesting an adverse reaction, increasing doses of aspirin (60 mg, 100 mg, 300 mg, and 400 mg) were administered until the patient developed a reaction. The same measurements were repeated every hour. Those having no history of aspirin hypersensitivity were started on 100 mg of aspirin, and this dose was gradually increased to 200 mg, 350 mg, and 450 mg until the patient developed a reaction. If no reaction occurred 4 h after the final dose, the test was deemed negative. Aspirin-induced bronchospasm, reflected by a decline (%) in FEV1, was calculated as the pre-challenge FEV1 minus the post-challenge FEV1 divided by the pre-challenge FEV1. Based on the OAC reactions, AERD and ATA groups were categorized as follows: (1) 15% or greater decrease in FEV1 or nasal reactions (AERD group), and (2) less than 15% decrease in FEV1 without naso-ocular or cutaneous reactions (ATA group). Peripheral venous blood was collected before the aspirin challenge.
SNP selection and genotyping
Four common ATF6B SNPs were selected based on minor allele frequency (MAF) >0.05 and LD status, from Asian populations in the International HapMap Project database (http://hapmap.ncbi.nlm.nih.gov/index.html.en). In the case of completely tagged SNPs (r2=1), only one was selected after considering location (e.g., functionally important SNPs were preferred). SNPs were then genotyped in 93 AERD and 96 ATA subjects using a Taqman assay, with assessment of data quality based on duplicate DNAs (n = 10). SNPs that could not satisfy the following criteria were excluded: (1) a minimum call rate of 95% for the accuracy of determining genotypes, (2) no duplicate error, and (3) HWE of P-value >0.05.
Statistics
We examined Lewontin's D' (|D'|) and the LD coefficient r2 between all pairs of biallelic loci to determine LD among the SNPs. LD was obtained using the Haploview v4.1 program downloaded from the Broad Institute.15 Haplotypes were first estimated using PHASE software,16 and then computed by logistic analysis using the Statistical Analysis System (SAS) v9.2. Associations were analyzed using logistic models with age (continuous value), gender (male = 0, female = 1), smoking status (nonsmoker = 0, ex-smoker = 1, smoker = 2), and atopy (absence = 0, presence = 1) as covariates. The effective number of independent marker loci was calculated to correct for multiple testing using the software SNPSpD (http://genepi.qimr.edu.au/general/daleN/SNPSpD/), which is based on the spectral decomposition (SpD) of the matrices of pair-wise LD between SNPs. The beta values indicating the effect sizes of differences in mean FEV1 among the genotypes of each SNP and haplotype were analyzed using the SAS. Statistical powers were calculated using the Power for Genetic Association Analyses (PGA) software,17 which is designed to calculate statistical power and other values in case-control association studies. For these measurements, the co-dominant (1df) model with a disease prevalence value of AERD 21%,3 effective degree of freedom (EDF) 2, and an alpha error level of 5% was used.
RESULTS
Characteristics of study subjects
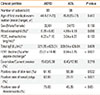
The clinical profiles of the study subjects are summarized in Table 1. A total of 189 asthmatic subjects were divided into 2 groups (93 AERD patients and 96 ATA controls) according to their records of FEV1 decline by aspirin provocation. The percentage of FEV1 decline and positive rate of nasal polyps and rhinosinusitis in AERD patients were higher compared to ATA controls (P<0.05). However, no significant differences in blood eosinophil, PC20 methacholine, total IgE, smoking status, and positive rate of skin test were found in the subgroups of this study (P>0.05).
Genotyping and haplotypes of ATF6B polymorphisms
Four common ATF6B SNPs with minor allele frequency (MAF) > 0.1, one in the promoter region, one in the coding region, and two in the 3'-untranslated region (UTR), were selected on the basis of their frequencies in Asian populations (Chinese and Japanese) from the International HapMap Project (Table 2, Fig. 1A). All alleles were successfully genotyped with an average call rate of 99.5% as shown in Table 2. The data reveal no significant departures from Hardy-Weinberg equilibrium (HWE) in any of the loci (P>0.05, Table 2). Four SNPs constituted four haplotypes with tight LD (Fig. 1B and C). Since ATF6B-ht2 and ATF6B-ht3 were equivalent to rs8283 and rs3830076, respectively, only ATF6B-ht1 and ATF6B-ht4 were included in the association analysis (Fig. 1B).
Associations of ATF6B polymorphisms with FEV1 decline by aspirin provocation and AERD
Interestingly, two SNPs (rs2228628 and rs8111) were significantly associated with % decline of FEV1 induced by aspirin challenge in the asthmatics (P=0.008 under the recessive model, Table 3), even after corrections for multiple testing (Pcorr=0.03). Minor homozygotes of rs2228628 and rs8111 showed about a 2.5-fold increase in the mean decline of FEV1 compared to the major homozygotes and heterozygotes (Table 3). In the haplotype analysis, ATF6B-ht4 was also significantly associated with FEV1 decline in the asthmatics (P=0.005 and Pcorr=0.02 under the recessive model, Table 3). At rs2228628, rs8111, and ATF6B-ht4, FEV1 declines were greatest for the homozygotes of the minor alleles (Table 3). However, logistic analysis adjusted for age, gender, smoking status, and atopy as covariates revealed no significant associations between ATF6B SNPs/haplotypes and the risk of AERD (P>0.05, Table 4). In further comparison of FEV1 decline by aspirin provocation between AERD and ATA groups, the strength of association with rs2228628 and rs8111 was increased in the AERD group (P=0.006-0.007 and Pcorr=0.02 under the recessive model, Table 3), but no association was observed in the ATA group.
In silico analysis of rs8111 in 3'-UTR
This study employed in silico analysis to predict potential function of the significantly associated rs8111 in the 3'-UTR. The UTRScan program (http://itbtools.ba.itb.cnr.it/utrscan), using a collection of sequences and regulatory motifs of the untranslated regions of eukaryotic mRNAs, revealed that 2 regulatory elements (the cytoplasmic polyadenylation element (CPE) involved in the polyadenine tail extension and mRNA activation for protein translation, and the upstream open reading frame (uORF) involved in interference with the expression of a downstream primary ORF) were discovered to include the rs8111 polymorphic site (Supplementary Table 1).
DISCUSSION
This study suggests that two SNPs (rs2228628 and rs8111) of ATF6B are significantly associated with FEV1 decline following aspirin provocation in AERD. In particular, this effect was significantly higher in minor allele homozygotes compared to major allele homozygotes and heterozygotes indicating that this allele plays a role in airway obstruction and leads to AERD susceptibility. Although actual functions of the heterozygotes remain to be validated, this result is attributed to the possibility that the heterozygotes of rs2228628 and rs8111 may display the ATA phenotypes rather than AERD.
Despite the fact that synonymous SNPs do not alter amino acid residue, several studies have revealed their functional associations with human diseases. Previous studies have also reported the associations of synonymous SNPs in the peroxisome proliferator-activated receptor (PPAR) gene (rs3856806, His 446His).18 In addition, the SET binding factor 1 (SBF1) gene (rs1053744, Thr1853Thr), discodin, CUB and LCCL domain containing 2 (DCBLD2) gene (rs828616, Ile262Ile) and leucine rich repeat containing 43 (LRRC43) gene (rs11060167, Arg 145Arg) were also observed to be associated with the risk of AERD.19 This previous evidence and our finding in this study suggest that a synonymous SNP in ATF6B (rs2228628, Ser201Ser) could affect FEV1 decline by aspirin provocation in asthmatics.
One possible explanation for the functional synonymous variant is suggested by the differential codon usage. More recently, codon bias using the relative synonymous codon usage (RSCU) has been reviewed within 50 genes from each of 9 species, including human. The results showed that Ser_TCC and Ser_TCG might exhibit a significantly different pattern of codon usage within the human genes (Supplementary Fig. 1),20 suggesting that codon usage and its adaptation to cellular tRNA abundances may lead to differences in gene expression and subsequent disease susceptibility. In addition, although no RSCU effect on the airway tissue has been reported, information about tissue-specific codon usage of Ser_TCC and Ser_TCG and their frequencies (Supplementary Table 2)20,21 suggest that codon-mediated translational control may play a role in the regulation of obstructive phenotypes in response to aspirin exposure in adult asthmatic patients.
This study also found that rs8111 in 3'-UTR was associated with FEV1 decline by aspirin provocation in asthmatics. The 3'-UTR SNPs usually affect protein expressions by altering the stability and secondary structure of mRNAs.22 In addition, results of in silico analyses in this study revealed that CPE and uORF elements, which include the rs8111 polymorphic site, were observed to be regulatory motifs in ATF6B. As for the functions of these 2 elements in the 3'-UTR region, CPE has been reported to act as a regulator for CAP-dependent translation,23 and uORF is involved in the mRNA translation during oocyte maturation and neuron development.24
The ATF6 protein, including ATF6B, is an ER membrane-bound transcription factor. ATF6 is a kind of transducer for the unfolded protein response and is activated by ER stress induced proteolysis.25 The ATF6 cascade induces appropriate folding and ER-association degradation of proteins by the transcriptional up-regulation of ER chaperone genes.26 ATF6B has five N-linked glycosylation sites, and its glycosylation is involved in ER stress induced proteolysis that cleaves 110 kDa ATF6B. It subsequently produces a nuclear form of 60 kDa ATF6B, which eventually moves to the nucleus and performs a repressor function to ATF6α (the other ATF6 isoform)-mediated ERSR by binding to various ER stress inducible promoters. A fully unglycosylated mutant of ATF6B was elucidated not to be cleaved, thereby leading to modulations of ERSR gene expression by losing its repressor function to ATF6α.10 Thus, the function of ATF6B may have a crucial role in ERSR, which has been implicated in inflammation related to airway disease.27 Recently, it has been suggested that ER stress can be induced not only by the alteration of protein folding but also by a decrease in Ca2+ concentration within the ER.6 In addition, NF-kappaB, which is involved in the activation of ER stress, showed a higher expression level in chronic obstructive pulmonary disease (COPD) patients who suffer from significantly lower FEV1 than healthy individuals.28,29 Therefore, it is suggested that ATF6B may play a role in pulmonary and allergic diseases through possible relations to the dysregulation of ER Ca2+ concentration and NF-kappaB.
In conclusion, two ATF6B SNPs (rs2228628 and rs8111, located in the coding region and 3'-UTR, respectively) were found to be significantly associated with FEV1 decline by aspirin provocation in asthmatics. In spite of several limitations such as lack of normal controls and no functional evaluation, our preliminary findings in this study could aid in developing a new strategy for the control of aspirin hypersensitivity in asthma.




 XML Download
XML Download