

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Micronutrient malnutrition and its adverse health outcomes are still prevalent, especially in the developing world [1], constituting 7% of global burden of disease with a cost of US $180 billion per year [2]. Deficiencies of the "big four" micronutrients, i.e. Vitamin A, Iodine, Iron, and Zinc, are still affect billions of people, particularly women and children. Despite considerable progress in eliminating these deficiencies through supplementation dietary diversification, and fortification, which were advocated for a long time, the goal is still far from being reached [3]. This has led to new approaches to improve micronutrient intake levels via biofortification, which is a strategy to enhance micronutrient concentrations in staple crops through conventional or transgenic breeding techniques. This potential strategy could radically reverse malnutrition if adopted and accepted by different populations [45].
The present study is the first to apply protection motivation theory (PMT) to analyse the potential adoption of biofortified foods as a means to tackle micronutrient deficiencies. The initial PMT model consists of three core constructs. Protection motivations (intention) are determined by the 'threat appraisal' and 'coping appraisal' components [678]. Threat appraisal consists of 'perceived severity' of the health threat, 'perceived vulnerability' of the person affected by the health threat, and 'perceived fear' of the effect of the threat [9]. 'Coping appraisal', on the other hand, consists of response-efficacy, self-efficacy, and the 'response cost'. Response efficacy describes how the health-promoting behaviour can minimize the health threat while the response cost describes the cost incurred by performing the recommended behaviour (negative to coping appraisal). 'Self-efficacy' refers to the individual's belief that they will succeed in the recommended behaviour to cope with the health threat. Previous research has mostly used part of the model and identified fear, severity, vulnerability, self-efficacy, response efficacy, and response cost as crucial in predicting intention and behaviour [8910]. Although the PMT Model was initially perceived as a model providing a clear understanding of fear appeals [11], it soon became a general theory of persuasive communication explaining cognitive processes that mediate (health) behavioural changes [6]. As such, it has been successfully applied to many health promotion activities [712]. According to a meta-analyses by Milne et al. and Floyd et al. [712], applications of PMT broadly fall into six topics: cancer prevention (17%), exercise/diet /healthy lifestyles (17%), smoking (9%), aids prevention (9%), alcohol intake (8%), and medical treatment adherence regimens (6%). In more recent studies, attempts have also been made to use this theory for predicting consumers' intention to consume functional foods and supplements [13141516]. No studies yet have applied this theory for predicting micronutrient-enriched foods. By using iodine biofortified lentils (IBVL), this study applies the PMT model to predict stakeholders' intention to protect children against iodine deficiency by consuming biofortified foods.
Iodine is an essential trace element found in seafood, iodized salt, and certain vegetables and is an important component of thyroid hormones, which generally determine human metabolic rate and promote growth and development throughout the body, including the brain, bones, skin, nerves, nails, and teeth [17]. Iodine deficiency mainly results in overgrowth of the thyroid gland, known as goitre, and long-term leads to a spectrum of diseases commonly referred as Iodine Deficiency Disorders (IDD). Iodine directly impacts the cognitive development of infants, pre-school, and school-aged children [18]. Iodine deficiency could prevent children at different levels from attaining their full intellectual potential and subsequently overall school performance [19]. As a consequence, two stakeholder groups, parent and schools, who are directly involved in determining meal composition and therefore iodine uptake at both the household and school levels are the focus of this study.
There is large evidence that these disorders can be corrected by adequate dietary supply of iodine [31820]. Iodine deficiency is a major health problem affecting both developing and developed countries due to its irregular distribution on the earth's crust, accelerated deforestation, soil erosion, and leaching processes [21]. Given the critical role of iodine in human nutrition [22], salt, oil, flour water, and milk iodization have been implemented over time to improve dietary iodine intake [23]. Although these efforts were very successful in some areas, the problem still remains in other areas of developing countries, particularly for people who live in remote mountainous areas, consume traditional vegetables high in salt (vegetarians), and land locked regions far from water masses [123]. Based on these risk factors, Eastern Africa was selected as the study location. Being one of the least developed regions of Sub-Saharan Africa, this region is remote and landlocked with limited access to seafood and iodized salt, which are key sources of iodine. Iodine deficiency is estimated to be 2.4% in Kenya, 4.2% in Uganda, and 41.5% in Tanzania [24]. These levels are considered to be due to populations that do not have access to existing strategies of salt iodization and are concentrated in rural landlocked locations. Therefore, this study evaluated the potential preferences for biofortified foods as an alternative health protection strategy to improve iodine intake in children. Iodine biofortified crops refer to crop materials that have been modified to enhance iodine content and thereby increase dietary iodine when consumed.
SUBJECTS AND METHODS
Data collection
Using multi-stage cluster sampling, data from three remote, rural landlocked locations in East Africa (Kenya, Uganda, and Tanzania) were collected. These locations were identified based on iodine status of the population using the latest data from the International Council for the Control of Iodine Deficiency Disorders (ICCIDD). The protocol used for this study was approved by respective authorities in Kenya, Uganda, and Tanzania.
The first stage of sampling involved selection of schools, representing clusters, using a regional list of schools in each country as the sampling frame. In total, 120 schools participated in the study, with 40 from each location. These clusters were then used as proxies from which nine households within the neighbourhood were randomly sampled (second stage), resulting in a total of 1,080 households with 360 per location.
Due to the focus on two target groups, i.e. schools versus households, data were collected by using two types of questionnaires: one for school heads and another for household heads (responsible for food purchases). Although both questionnaires focused on children (home versus school consumption) and consisted of five common blocks (knowledge, information, iodine status, PMT and behaviour, and socio-demographics), there was a slight variation between both in the sense that school heads answered from the school perspective (e.g. school feeding programme) while the household questionnaire collected data on the household level.
The questionnaire was pretested with randomly selected representative households (N = 10) and schools (N = 5).
Questionnaire
Both survey questionnaires consisted of five parts: a) knowledge about iodine, iodine deficiency disorders, prevention strategies, and biofortification; b) iodine intake status; c) IBVL (information); d) Protection Motivations and actual behaviour (as preferences and reflected as willingness-to-pay element). The main questions were derived from previous applications of the PMT model in examining health-related dietary behaviours [71215] and adapted to the case of iodine biofortified vegetable legumes to identify determinants influencing consumption of foods with high iodine contents to prevent iodine deficiency disorders and related conditions. The message characteristic was based on four constructs of PMT that dictate intention and consumption behaviour: severity of iodine deficiency disorder and related health problems (severity), vulnerability of the target group to the deficiency (vulnerability), efficacy of the proposed behaviour to avert the deficiency (response efficacy), and efficacy of the group to perform the presented behaviour to prevent the deficiency (in this context, consumption of iodine biofortified foods). All items of the applied PMT model were measured by a 5-point Likert scale (strongly agree to strongly disagree; extremely unlikely to extremely likely).
Two dependent variables were considered for this study: protection motivation (intention) to consume IBVL and protection behaviour (IBVL consumption behaviour).
The original dependent variable of the PMT model, i.e. intention to engage in a health-related behaviour (protection motivation), was adapted from previous research [1325] and represents participants' intention to accept, advocate, buy, as well as include IBVL in household or school meals. Furthermore, protection behaviour was represented by a willingness-to-pay question using a premium card procedure that measures a premium or discount. Responses were converted into categorical data (1-5). Assessment of protection behaviour or behaviour towards IBVL hinged on the definition of behaviour formulated and presented by Ajzen [26], who refers to using Target, Action, Context, and Time (TACT) elements to define behaviour as a manifest, observable response in a given situation in reference to a given target. Therefore, willingness-to-pay (WTP) for an attitude change, which was successfully applied in previous studies [27], was measured. TACT elements were adapted to our case, i.e. IBVL (target); willingness-to-pay (action); local market and school settings (Context); and offering a premium or discount (Time), and combined with a contingent valuation approach using payment cards. Five items were used to assess behaviour, based on the following statements: "If normal vegetable legumes cost US $1.5 (put in local currency) and biofortified vegetable legumes US $1.75-2.25, how much are you willing to pay for iodine biofortified vegetable legumes without viewing them expensive? Biofortified vegetable legumes…US $", "Considering the normal school meal cost US $1/day (put in local currency), and biofortified US $1.5-2, how much more are you willing to pay for inclusion of iodine biofortified vegetable legumes in school meal. Iodine biofortified vegetable legume in school mea l…US $". The normality of the responses was then calculated to determine the reliability of the data for further analysis.
As previous research has demonstrated that consumption of functional foods, biofortified foods, and other health materials is a function of many determinants that are not included in the original PMT model, such as price, knowledge, information, and nutrition status [2829], and that consumers are not likely to comprise key attributes of the product for health [29], we introduce these exogenous factors in our extended PMT model (Fig. 1).
The questionnaire was pretested with randomly selected representative households (N = 10) and schools (N = 5).
Data analysis
We used the EpiData platform to enter the data. EpiData enabled error detection, such as double entry verification as well as data coding. All data were analysed using STATA.
Cronbach's alpha was calculated to determine reliability of the items of the original PMT model, and only items with an α > 0.6 qualified for inclusion in the study. The responses for protection behaviour (continuous variables) were treated as continuous variables to determine the participant's WTP when IBVL are offered at a premium and at a discount. Using these two scenarios, Maximum Likelihood range WTP modelling was performed to estimate the final willingness to pay for IBVL.
Pathway analysis modelling (PAM) was conducted to identify the underlying effect of dependent variables on the WTP for IBVL. Pathway analysis modelling is often a form of structural equation modelling [30] and is an extension of the general regression model used to test the fit of the correlation matrix against causal models or relationships, which are of interest [3031]. In the current study, the model was applied to test the fit of the correlation matrix or relations between endogenous and exogenous variables within the PMT model as well as their subsequent effect on WTP for IBVL. Regression was carried out for each variable as a dependent variable of all other variables included in the study [3132], which are believed to be causative: threat appraisal, coping appraisal, and protection motivations (intention). More often than not, the model is particularly sensitive to model specifications and therefore requires adherence to the usual regression assumptions [32]. The model attempts to: 1) understand patterns of correlation among the variables and 2) explain this level of variation as much as possible within the specified model. It is often distinct from other statistical testing techniques such as multiple regression and ANOVA, in that it mainly focuses on a decision about the whole model with three expected outcomes: reject, modify, or accept [33].
In the current study, pathway analysis modelling was undertaken at three different levels: "protection motivations (intention) to consume IBVL)" as the dependent variable with endogenous (PMT) variables and exogenous variables as the independent variables (1); "protection behaviour" (WTP) as the dependent variable with all other variables together and the primary variable (intention) as the independent variables (2); similar to the second level but using WTP as a dummy variable. Thereby, goodness of fit for the model was analysed using RMSEA.
Before running the model on the entire dataset, it was applied for each gender and country to detect any significant variations.
We also conducted Tobit modelling to determine the likelihood levels of each element presented in the path analysis with regard to the willingness to pay for IBVL. The Tobit model, which also censors regression modelling, is a type of model designed to estimate the overall linear relationship between variables when there is either left or right-sided censoring of the dependent variable [3435], also known as censoring from below and above, respectively [35]. In the current study, censoring from above means willingness-to-pay lower than the market price of the product (discount), whereas censoring from below means willingness-to-pay above market price (premium). All variables are then modelled around each censoring to determine their relation with the final value [36], which is the case for WTP. This procedure often allows for amelioration of biased coefficients in the model, when WTP is subject to changes due to diversity in consumer segments [3436]. Although Tobit modelling is superior to classical analysis of multidirectional data, its limitations and appropriate applications are an important consideration which informed use in the current study [36].
RESULTS
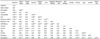
Sample descriptions are presented in Table 1. Two samples were successfully recruited from each of the three countries at the school (40 participants) and household levels (360 participants). Based on the targeted stakeholder, our sample consisted of 1080 (households) and 120 respondents (schools). In both samples, a Cronbach's alpha (α) value above 0.60 was reported for all variables, which justifies the development of composite variables.
The two samples collected were different in many respects and, as expected, socioeconomic status and education level of school heads were higher than those of parents. In both cases, most of the participants were males: 53.8% and 65.83% at the school and household levels, respectively. As expected, males were more involved in managing schools. There were small age differences between both samples. The high number of children in households, on average six per household and about 650 per school, indicates that this was a highly populated region. Among the participants, an average of two members per household and a total of 297.38 were children aged 6-12 years who showed high susceptibility to iodine deficiency disorders. Low income and education levels at the household level underline the socio-economic challenges in these regions. The average school performance of children in households was 59.82% (SD ± 17.82) and 56.5% in schools. Despite the negatively perceived performance of the children, satisfaction level (1-5) of the respondents at the household level was twice as high than at the school level. Regular consumption of food through function school feeding programmes was common, with households indicating that their children consumed food at school more than three (SD ± 1.87) times a week while school heads indicated school feeding programmes in operation for more than 2 years on average.
Regarding PMT components, respondents at the household level reported higher values (above 4 on a 1-5 scale) for severity, vulnerability, fear, response efficacy, self-efficacy, and protection motivation than school heads. However, the response cost was slightly higher at the school level.
The preferences, in form of willingness-to-pay (WTP), of household and school heads in regard to IBVL was examined against regular vegetable legumes. Given that the latter cost US $1.5, WTP for IBVL was US $1.89 (SD ± 0.17) and US $1.84 (SD ± 0.17) at the household and school levels respectively, when offered at a premium. However, values were slightly lower when respondents were asked if they are willing to pay to include it permanently in the school feeding programme, i.e. US $1.72 and US $1.67 for household and school heads, respectively. Moreover, when examined as a discount, respondents at the household level were eager to accept a larger discount (US $0.98) than at the school level (US$ 1.01). Values were even lower when respondents were asked to include IBVL in the school feeding programme, US $0.67 and US $0.63, respectively.
Table 2 contains the bivariate correlations between all study variables that are inserted into the path analysis model of the household sample. There were weak to strong positive correlations between protection motivations (behavioural intention) to consume IBVL moderate positive correlations and the following PMT model variables, including severity (38%), vulnerability (37%), fear (46%), response efficacy (39%) and self-efficacy (56%). Nonetheless, the protection motivations (behavioural intention) was negatively correlated to the occupation of the respondents (-18%).
Path analysis modelling
The results of path analysis modelling, which describes the directed dependencies among the study variables, are displayed in Table 3. The model links exogenous variables (knowledge, socio-demographic indicators, and iodine status) to endogenous (PMT) variables (threat and coping appraisal elements) and subsequently to the dependent variable (protection motivations, also behavioural intention). Two exogenous variables, knowledge and occupation, significantly influenced the intention of households to consume IBVL. Furthermore, severity, fear, and self-efficacy significantly predicted intention to consume IBVL. However, threat appraisal was a function of individuals' iodine status, the presence of vulnerable children in the household, response efficacy, response cost, and self-efficacy. On the other hand, coping was influenced by iodine status, severity, vulnerability, and fear. In other words, threat appraisal influences coping, and vice versa, in order to increase uptake of IBVL.
At the school level, the intention to consume or include IBLV in school feeding programmes is mainly a function of vulnerability and self-efficacy. In addition, the targeted country significantly influenced threat appraisal, whereas no significant effects were observed regarding coping appraisal. All potential determinants of the intention to consume IBVL were included in two-limit Tobit modelling to determine their effects on WTP for IBVL at the school and household levels.
Two-limit tobit modelling
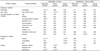
Table 4 shows the results of a series of two-limit Tobit regression modelling, in which the dependent variable is WTP for IBVL as a protection behaviour, censored at the premium or discount level.
The analysis elucidated highly significant effects of protection motivations (P < 0.001), severity (P < 0.001), and gender (P < 0.01) towards IBVL when offered at a premium. However, when asked about their willingness-to-pay to include IBVL into the school feeding programme, when offered at a premium, response efficacy and the country of the household were the most significant elements. Furthermore, protection motivations and response cost were very significant when IBML was presented at the school level. On the other hand, protection motivation is only significant when IBVL was included in a school meal, whereas the response cost was only significant when IBVL was permanently included in the school programme.
When IBVL was presented at a discount, severity, fear, response-efficacy, and iodine status had significant effects on preference of IBVL in household meals. Additionally, preference of the household to include IBVL in the school programme is determined by perceived vulnerability to IDD and response efficacy of the alternatives provided, as well as age, gender, decision maker, and the country of the respondent.
However, at the school level, WTP for IBVL offered at a discount is a function of perceived vulnerability and fear of IDD in addition to age and gender. Furthermore, inclusion of IBVL in the entire feeding programme is dependent on severity, response efficacy of the proposed alternatives, knowledge about IDD and biofortification, as well as the age of the respondent. In principal, our model has a significant degree of fit and maximum level of willingness-to-pay for IBVL.
DISCUSSION
The aim of the current study was to analyse how well factors exogenous and endogenous to the PMT model predict protection motivations (intention) and subsequent protection behaviours (consumption). The study presents a case of IBVL to protect households and their children from iodine deficiency disorders and improve school performance of children. Over the years, knowledge about nutrients and nutritious foods, such as biofortified foods, and their links to health has been insufficient [37]. Although attempts have been made to draw significant associations between nutritional knowledge and nutrient intakes, very few studies have demonstrated these links, and significance levels are far from being realized [1438]. The findings of the current study are no different. Knowledge about iodine, its link to iodine deficiency disorders and poor school performance, as well as available prevention strategies such as salt iodization and biofortification was insufficient and lower in less educated than highly educated groups. The responses regarding a set of questions evaluating nutritional knowledge about micronutrients, iodine, iodine deficiency, salt iodization, and biofortification differed significantly between different groups. Nutritional knowledge of less educated household respondents was relatively low compared to more educated respondents at the school level. Fig. 2(A) shows that knowledge about iodine, health threats arising from deficiency of iodine, and the subsequent novel strategy of food biofortification was very insufficient. Nevertheless, many previous studies have presented elements that largely account for the low influence of nutritional knowledge on dietary changes to increase nutrient intake for health and nutrition well-being [3839]. These findings demonstrate the likely importance of including nutritional knowledge in designing health education campaigns, particularly in the prevention of iodine deficiency disorders and poor school performance, through novel strategies such as biofortification. Knowledge about nutrient-related deficiency disorders and approaches for preventing these disorders are very important elements for consideration [40].
Furthermore, for nutritional education campaigns to be successful, it is worth considering the types, sources, and modes of communicating nutritional messages such as nutrients, sources, health threats, and available prevention mechanisms [41]. Fig. 2(B) demonstrates that the market, media, and professionals are the most effective avenues. Even though media is effective in highly educated groups such as school heads, use of professionals and markets are more effective in less educated groups such as households.
In predicting protection motivations (intention) to consume biofortified foods (IBVL) as a means of preventing IDD and improving school performance of children, the study results provide some support for endogenous and exogenous elements in the PMT model. At the household level, in contrast to our hypothesis, only two exogenous elements, knowledge and occupation, and three endogenous elements, severity, fear, and self-efficacy, were able to directly and significantly predict protection motivations (intention). Accordingly, iodine status and presence of young children (6-12-years-old) indirectly predicted behavioural intention through 'threat' appraisal and 'coping' appraisal. Further, at the school level, in contrast to our hypothesis, only two endogenous, vulnerability and self-efficacy, and one exogenous variables, country of origin, significantly predicted intention to consume IBVL.
These findings are consistent with results from earlier studies predicting intention and interventions in health behaviour, particularly dietary behaviour [7]. Self-efficacy, an endogenous element of the coping appraisal construct of PMT, was found to be the most important predictor of intention to consume biofortified foods at both the household and school levels. This is consistent with earlier studies predicting dietary behaviours regarding nutritious foods that reported self-efficacy as a decisive factor in nutritional education campaigns for dietary changes [141542]. However, severity, fear, and vulnerability from the PMT threat appraisal construct as well as exogenous elements knowledge and occupation had direct and significant effects on intention of biofortified foods. Still, other exogenous elements such as iodine intake status and presence of young children aged 6-12 years had significant effects, albeit indirectly.
These findings point to a more pronounced effect of threat appraisal combined with exogenous elements, which differs from earlier studies that demonstrated 'coping' appraisal as having the most important effect on intention to consume and nutritious foods [1415]. Therefore, it is a precarious undertaking to ignore 'threat' appraisal as well as exogenous elements in the prevention of micronutrient deficiencies through biofortified foods such as IBVL. The combined effect of these elements is highly significant and important, which contradicts the conclusion that self-efficacy is the most important in health and nutritional promotion. Therefore, to increase protection motivations (intention) to consume a healthy diet or nutritious foods such as biofortified foods, communication of the 'threat' appraisal and exogenous elements is worthwhile. Programmes targeted to vulnerable groups both at the household and school levels (school feeding programme) should include these elements in their nutritional promotion campaigns and in launching novel preventive strategies such as biofortification.
The focus of the path analysis modelling in the current study was to assess elements that influence and predict protection motivations (intention) to consume nutritious foods, particularly biofortified foods. However, two-limit Tobit modelling (Table 4) was used to evaluate the effect of endogenous and exogenous variables to the PMT model that influence protection behaviours or preference for adopting biofortified foods (in this case IBVL). The preference was presented as a willingness-to-pay component when the biofortified product was offered at a premium or discount at both the school and household levels. An attempt was also made to examine the elements influencing preference for this product for inclusion in a school feeding programme.
Results from Table 1 show that households are willing to pay an average US $1.89 (premium, US $0.39) and US $1.72 (premium US $ 0.22) for IBVL meal and inclusion of IBVL into a school feeding programme to protect their children. Consequently, school heads are willing to pay US $1.84 (premium US $0.34) L and US $1.67 (US $0.17) for IBVL and inclusion into a school feeding programme, respectively. However, when the product was offered at a discount, parents were willing to pay US $0.98 (discount, US $0.52) and US $0.67 (discount US $0.83) for IBVL and inclusion into a school feeding programme, respectively. These results demonstrate a willingness to pay a premium and acceptance by both the parent and school for accruing nutritional benefits. This is consistent with earlier studies examining willingness-to-pay for foods with health benefits, particularly nutritional benefits [3843444546]. Respondents were willing to accept fewer discounts when the iodine biofortified product was offered at a discount due to the envisaged nutritional benefits, albeit more at school level than in households due to the attachment of children to their parents.
Table 4 shows results from the Tobit model. A total of two sets of Tobit models were developed. First, model estimated exogenous and endogenous PMT variables influencing preference for IBVL when offered at premium. Protection motivations (intention) were the most important factor that directly and significantly influenced willingness-to-pay for iodine biofortified foods at both the household and school levels. At the household level, other elements, severity, and gender were very significant. However to include the product into school meals, response (product) efficacy and country of the household are important at the household level, whereas response cost was important at the school level. These results are in tandem with previous findings examining the link between protection motivations (intention) and actual protection behaviour (preference as defined by willingness-to-pay) in regard to health intervention (in this case Biofortification) [6816]. Therefore, these elements should form part of health and nutritional promotion programmes for prevention of micronutrient deficiencies, in this case IBVL for iodine deficiency and improved school performance. For instance, households are likely to pay a premium to protection their children from iodine deficiency disorders and improve their performance if nutritional campaigns communicate the severity of the threat, and mothers are more involved and their motivation towards the proposed product is high. In essence, schools are likely to pay more when convinced that proposed behaviour will protect their children against iodine deficiencies and improve school performance. Second, a model evaluated exogenous and endogenous PMT variables influencing the preference for IBVL offered at a discount at both the household and school levels. Severity, fear, response efficacy, and iodine status were the most important and significant factors influencing preference for IBVL when offered at a discount to households. When the product was offered at a discount at the school level, vulnerability, fear, gender, and age were the most significant factors. However, for inclusion of the product into the school feeding programme, households are likely to accept that it can be significantly influenced by vulnerability, response efficacy gender, age, decision maker of the household, and the country in question. While the amount of discount schools are likely to accept in order to include the IBVL into the school feeding programme, in the long-term is a function of severity, response efficacy, knowledge level, and age of the respondent.
These findings are consistent with earlier results that have examined willingness-to-pay for nutritious foods (in this case biofortified foods), particularly in resource poor countries [434445]. When nutritious products were offered at a discount, the protection behaviour (preference) was shown to be a function of the health threat and socioeconomic factors such age, gender, and knowledge level. Consumers, at either the household or school level, were more likely to accept fewer discounts (pay more for the proposed prevention measure) if the health threat in question was more important to them and their children. Therefore, these elements should be incorporated into nutrition campaigns to be successful.
Although consumers are likely to pay for various discounts depending on the perceived value of the product and its health benefits, they are not likely to composite taste for health [29]. This points to the fact that households are more sensitive to health threat and are likely to accept a lesser discount in order to protect their children.
In principle our results extend earlier findings and contribute to the growing body of literature on the prevention of micronutrient deficiencies through biofortification. The findings point to the growing need to consider endogenous PMT variables, particularly 'threat' appraisal constructs as well as exogenous elements such as age, gender, and knowledge, in decision-making and in designing nutritional intervention campaigns for micronutrient deficiencies.
The preference (willingness-to-pay) and factors that influence this protection behaviour are very important in understanding the adoption of biofortification as a novel strategy in prevention of micronutrient deficiencies [4748]. This points to the importance of enhancing policies to build local markets and subsequent availability of these foods.
Since consumers are willing to pay more for biofortified products, such as IBVL, these findings are central to guiding policy formulation targeted to the entire agro-food chain as well as producers (farmers) and investors. Equally, the level of discount acceptable by consumers to protect themselves and their children through biofortification is fundamental to governments, investors, implementers of programmes, and donors in regard to the level of subsidy and policy framework necessary. In essence, the policy direction reflected from these findings points to the potential of biofortification in prevention of micronutrient deficiencies as well as growth of the rural economy around school feeding programmes.
Therefore, if IBVL have potential to minimize iodine deficiency and improve school performance in children, a systematic strategy should be formulated based on these and other findings, which hinge on the delivery system, particularly through school feeding programmes and household food consumption. The proposed delivery system should focus on pricing, marketing, and distribution and take into account protection motivations and preference (willingness-to-pay) at both the household and school levels.




 XML Download
XML Download