

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Pes planovalgus, or flatfoot deformity, is the most common foot deformity that can be difficult to define. The flat foot usually refers to a foot with a decreased medical longitudinal arch, but it is actually a three-dimensional deformity with hindfoot valgus, forefoot abduction, and supination.1234) There are diverse causes of flatfoot. Rigid flatfoot such as tarsal fusion, vertical talus, and pes planovalgus caused by neuromuscular disorders such as cerebral palsy can cause symptoms such as pain or gait disability. On the other hand, most cases of flexible flatfoot (FFF) do not cause symptoms, especially in children. However, pes planovalgus with short tendo-Achilles and hyper-mobile flatfoot are known to cause pain or other symptoms with increased activities and body weights.5678) These symptoms become more obvious after the age of 10 years and may last into adulthood.910)
Staheli11) described pes planovalgus as a common physiologic variant among children and is able to persist with a normal foot shape even among adults. They also pointed out that medial longitudinal arches tended to develop naturally along with the growth of children.12) Harris and Beath6) and Wenger et al.12) also concluded that FFF is a physiological deformity found during the normal development of children that often improves with growth. They also mentioned that FFF does not necessarily imply vulnerability of foot structures.
However, pes planovalgus with midfoot breakage and talonavicular subluxation is considered as a kind of lever arm disease by other authors.131415) The lever arm is shortened with forefoot abduction, and the lever becomes flexible with midfoot breakage in pes planovalgus. Theoretically, this may reduce energy efficiency by causing kinetic loss during gait. This study aimed to quantify the kinetic inefficiency of symptomatic flatfoot during gait by comparing the results of gait analysis of flatfoot patients and normal controls.
METHODS
Subjects
The patient group consisted of 26 children (50 feet, n = 50, including 2 children with unilateral involvement) with symptomatic flatfoot who visited the outpatient clinic from October 2005 to February 2014 and were studied with gait analysis. This study excluded children with flat-foot caused by neuromuscular diseases such as cerebral palsy and rigid flatfoot such as tarsal coalition and vertical talus. Twenty-one children were male (40 feet, n = 40), and 5 were female (10 feet, n = 10). The mean age was 9.5 years (range, 7 to 13 years). The mean height of patients was 135.7 cm (range, 126 to 162 cm) for male children and 138.6 cm (range, 133 to 146 cm) for female children. Male and female patients' mean weights were 36.3 kg (range, 21 to 62 kg) and 35.2 kg (range, 31 to 41 kg), respectively. The causes of pes planovalgus in the patient group were Achilles tightness (16 patients, 31 feet) and ligament laxity (10 patients, 19 feet) (Table 1).
The normal control group included 50 healthy male and female university students (100 feet, n = 100) who had fully developed medial longitudinal arches in their feet without any medical history of musculoskeletal disease. Volunteers for control group were checked with history taking, physical examination and lower extremity orthogram. We confirmed that the volunteers had no bony abnormalities or any musculoskeletal diseases and they have normal arched feet either in weight-bearing state or in non-weight-bearing state. The mean age of the control group was 21.3 years, and the mean height was 167.1 cm.
All procedures performed were approved by the Eulji University School of Medicine Institutional Review Board (No. EMC 2017-07-003-001), and were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from the legal parent/guardian of the participants included in the study.
X-Ray Measurement
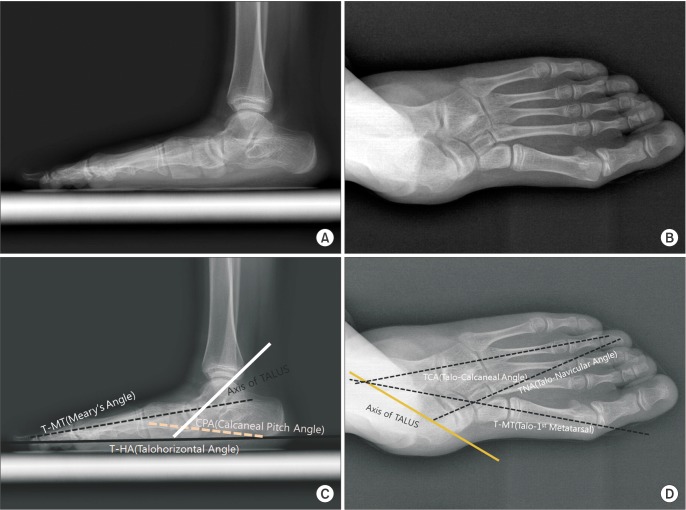
The severity of the static deformity in the patient group was evaluated with standing foot X-rays of the anteroposterior (AP) and lateral images (Fig. 1). The talocalcaneal angle, talonavicular angle, and talo-first metatarsal angle were measured on standing AP images of the foot. The talo-first metatarsal angle, talo-horizontal angle, and calcaneal pitch angle were measured on standing lateral images.
Gait Analysis
For gait analysis, history taking, physical examination, video imaging of walking, and three-dimensional motion capture for kinematics and kinetics were conducted. The patients' symptoms were assessed before gait analysis. The range of motion of each joint was measured using a goniometer, including the plantar flexion and dorsiflexion of the ankle joint. When measuring dorsiflexion, the foot was slightly inverted to lock the subtalar joint and avoid any subsidiary dorsiflexion at the subtalar joint. The amount of ankle dorsiflexion was measured with the knee extended (ankle dorsiflexion with knee extension [ADKE]) and flexed (ankle dorsiflexion with knee flexion [ADKF]).
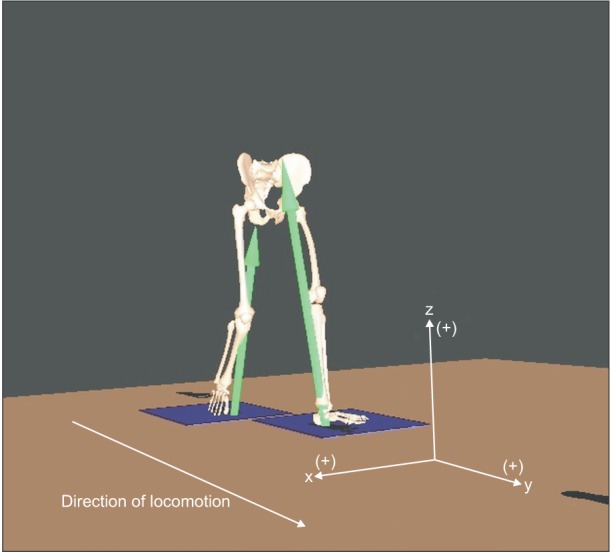
For three-dimensional motion capture, passive reflective markers were attached according to the modified Helen-Hayes marker set. The Eagle system (Motion Analysis, Santa Rosa, CA, USA) consisting of 6 digital cameras was used for optical tracking of the markers. The subjects' gaits were captured while subjects walked along a walkway (7 m long) several times at a comfortable speed. The frequency of the motion capture was set at 120 frames per second (120 Hz). EvaRT 5.0 (Motion Analysis) and Orthotrak 6.6 software (Motion Analysis) were utilized for data processing. The ground reaction force (GRF) was measured using the two AMTI force plates (AMTI, Watertown MA, USA), which were installed at the center of the walkway. GRF between the limb and the ground during the stance phase was measured using 2 AMTI force platforms by the technique of strain-gauging. Two AMTI force plates were embedded at the center of gait way, and the mean values of GRFs obtained after several walking in the gait lab was used for analysis. Theses measured kinetic vector values were integrated along with kinematic data using Eva-RT (Motion Analysis Corp., Santa Rosa, CA, USA) and Orthotrack software (Motion Analysis Corp.). Joint moment and power were also calculated by the inverse dynamics. The Euler angle coordinate system for measurement of GRF was set as Fig. 2.
Data Processing and Analysis
Results of the radiographic measurement, physical examination, kinematics, and kinetics in the patient group and control group were statistically analyzed using SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA). To compare the patient group and control group, an independent t-test was used with a p-value significance threshold of less than 0.05.
RESULTS
Physical Examination
The most frequently reported symptoms of the patient group were pain (8 cases, 16 feet), limping (abnormal gait of children; 15 cases, 29 feet), and limping with pain (3 cases, 5 feet) (Table 1). The average ADKF and ankle plantar flexion in the patient group were 19.3° (range, −10° to 40°) and 44.9° (range, 40° to 50°), respectively, with no significant difference from the control group. By contrast, the mean ADKE was 5.6° (range, −15° to 30°) for the patient group, which was lower than that of the normal control group (mean, 10°; range, −15° to 30°). This result reflects the fact that many subjects in the patient group had shortened Achilles tendons.
X-Ray Measurement
In the patient group, the mean AP talocalcaneal angle was 35.5° (range, 15° to 60°), the mean AP talonavicular angle was 24.0° (range, 7° to 48°), and the mean AP talo-first metatarsal angle was 20.2° (range, 2° to 42°) on the AP radiographic images (Table 2). On the lateral radiographic images, the mean talo-first metatarsal angle was 12.0° (range, 3° to 32°), the mean talo-horizontal angle was 30.7° (range, 22° to 45°), and the mean calcaneal pitch was 11.6° (range, 1° to 20°). These radiographic measurements reflected the presence of typical pes planovalgus of the patient group.
Kinematics
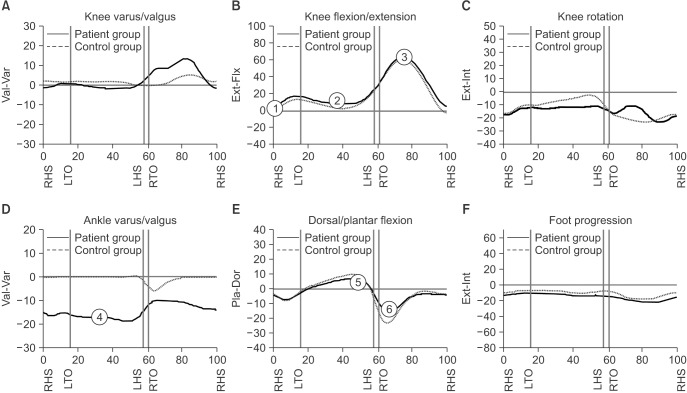
The most prominent feature of ankle joint kinematics in the coronal plane was the 17° of continuing heel valgus during the stance phase (Fig. 3D).
The degree of ankle dorsiflexion in the patient group did not significantly decrease during the period of the second rocker in the sagittal plane. The maximum ankle dorsiflexion (Fig. 3E) at the end of second rocker for the patient group (6.5° ± 9.7°) was not significantly reduced (p = 0.09) compared to the control group (9.4° ± 3.6°).
The degree of plantar flexion during the third rocker in the patient group was reduced (p < 0.05). This observation does not support our initial prediction that the amount of dorsiflexion might be reduced, and plantar flexion might be the same or greater in the patient group compared to the normal control group, as the Achilles tendon was tight in many cases in the flatfoot patients. The degree of maximum plantar flexion at the end of third rocker (Fig. 3F) was 13.1° ± 10.5° in the patient group and 19.2° ± 7.9° in the control group. The entire range of plantar flexion during the third rocker was 19.5° ± 8.8° in the patient group and 28.7° ± 7.5° in the control group. The entire range of plantar flexion in the patient group during the third rocker was significantly less than that of the control group (p < 0.05).
The knee joint of the patient group was more flexed, by approximately 5°–6°, over the whole gait cycle compared with that of the control group in the sagittal plane. The knee joints of the patient group were in a slightly flexed position of 6.6° on average at the initial contact of the stance phase (Figs. 1C and 3A); whereas, the knee joints of the control group were in fully extended posture at that point (p < 0.05). At the mid-stance phase (Fig. 3B), the knee was flexed 9.1° on average in the patient group and flexed 2.2° in the control group (p < 0.05). The knee position at peak knee flexion of the early swing phase (Fig. 3C) was 61° on average for the patient group and 58° on average in the control group (p < 0.05).
Kinetics
GRF
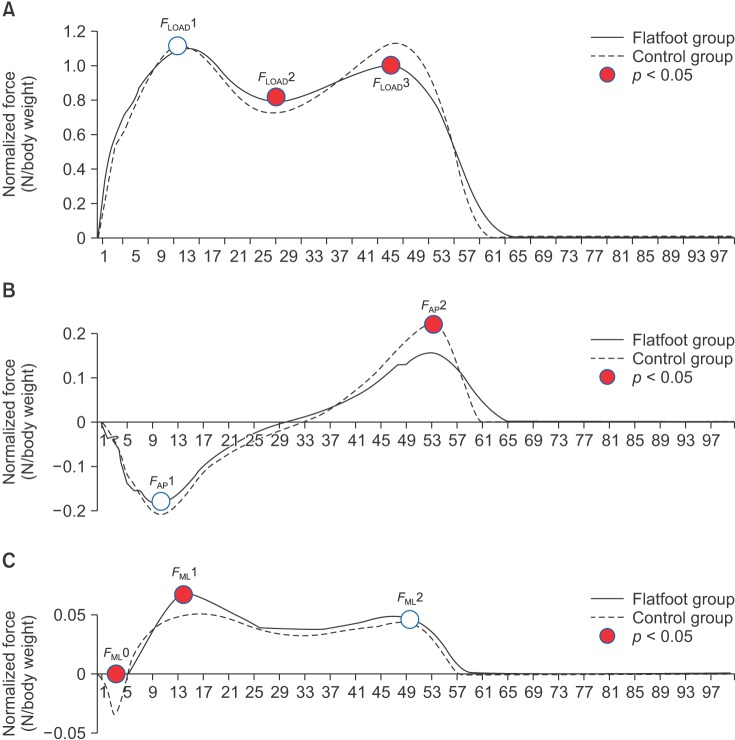
The direction and degree of the GRF vector in the stance phase were measured in three dimensions, and the measured values were normalized by the weight of each subject. In other words, the fore-aft shear force (GRF-FWD), medial-lateral shear force (GRF-LAT), and vertical shear force (GRF-VRT) were measured as components of the GRF vector in three dimensions. The values of the vertices of each graph were statistically compared between the patient group and the control group (Table 3).
Of the three vertices (FLOAD1, FLOAD2, and FLOAD3) on the GRF-VRT graph (Fig. 4A), FLOAD1 and FLOAD2 did not significantly differ between the 2 groups. FLOAD3 (the third vertex located at 47% of the gait cycle) was 0.99 ± 0.18 (N/body weight, normalized force) for the patient group and 1.15 ± 0.21 for the control group (p < 0.05). The GRF-VRT vector at the push-off period (FLOAD3) of the patient group was reduced compared with that of the control group.
The GRF-FWD graph (Fig. 4B) had 2 vertices: FAP1 (peak braking force) and FAP2 (peak pushing force). The mean FAP1 of the patient group was −0.18 ± 0.06, whereas it was −0.21 ± 0.04 for the control group (p < 0.05). FAP2 was 0.16 ± 0.05 and 0.22 ± 0.03 for the patient group and the control group, respectively (p < 0.05). Thus, the peak braking force and the pushing force of the forefoot rocker were reduced for the patient group.
The GRF-LAT graph (Fig. 4C) had three vertices: FML0 (a downward vertex at 5% of the gait cycle), FML1 (14% of the gait cycle), and FML2 (49% of the gait cycle). FML0 was −0.01 ± 0.02 and −0.03 ± 0.02 for the patient group and the control group, respectively (p < 0.05). FML1 was 0.07 ± 0.03 and 0.06 ± 0.02 for the patient group and the control group, respectively (p < 0.05). FML2 did not significantly differ between the two groups. The GRF-LAT was greater for the patient group, which was attributed to a hindfoot valgus alignment of the flatfoot deformity.
Ankle moment and power
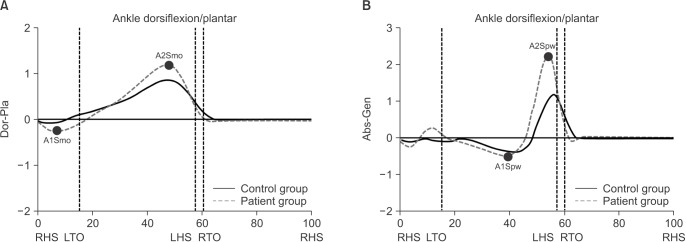
There were 2 peaks on the ankle moment graph in the sagittal plane: A1Smo, a downward peak during the loading response, and A2Smo, an upward peak during push-off. The minimum ankle joint moment in the sagittal plane (A1Smo, the first peak ankle moment in the sagittal plane) was −0.05 ± 0.11 for the patient group and −0.12 ± 0.13 for the control group (p < 0.05). The maximum moment (A2Smo, the second peak of ankle moment in the sagittal plane) was 0.89 ± 0.26 for the patient group and 1.27 ± 0.25 for the control group (p < 0.05) (Table 4 and Fig. 5). In other words, the internal dorsiflexion moment at the loading response and the peak plantar flexion moment at the terminal stance were lower in the patient group than the normal control group, and the reduction of the peak plantar flexion moment for the patient group was approximately 30% compared to that of the control group. This reduction reflected the inefficiency of the leverage system in patients with flatfeet.
The ankle joint power graph in the sagittal plane showed A1Spw, a downward peak at the region of power absorption (corresponding to eccentric plantar flexor activity at the ankle during the midstance and terminal stance) and A2Spw, an upward peak at the region of power generation (corresponding to the concentric burst of propulsive plantar flexor activity during pre-swing). The A1Spw was −0.36 ± 0.44 for the patient group and −0.41 ± 0.38 for the control group (p > 0.05), and the A2Spw was 1.38 ± 0.73 for the patient group and 2.52 ± 0.78 for the control group (p < 0.05). The mean value of ankle power was 0.04 ± 0.15 for the patient group and 0.14 ± 0.11 for the control group (p < 0.05) (Table 4 and Fig. 5). The power of concentric propulsive plantar flexor activity providing the forward momentum during the terminal stance and pre-swing phase was reduced by 45% compared to the value of the normal control group.
DISCUSSION
The ankle joints are a type of second-class lever. During the push-off at the third rocker, the entire foot becomes a lever (L) and lifts the body weight (R, resistance). Herein, the metatarsal heads become a fulcrum (P) and the Achilles tendon provides the effort (E). For the lever system to operate effectively, a lever should be solid rather than flexible and have an appropriate distance (d) between the fulcrum (P) and the effort (E). In addition, it should produce an appropriate amount of force through muscle contraction.
In symptomatic pes planovalgus deformity, the lever arm is shortened due to forefoot abduction and heel valgus, and the hardness of the lever decreases and becomes flexible due to midfoot breakage.124) It is necessary to generate a certain moment size for the gait in the ankle joint that corresponds to the second-class lever. If the length of a lever is shortened due to foot deformity, then it becomes imperative for muscles to generate an even stronger force (Fe, effort).
Many researchers have reported that pes planovalgus in children is a positive foot deformity found in the process of normal development; thus, it should not cause symptoms and eventually improve by itself. However, pes planovalgus is a type of lever disability from the perspective of kinetics; thus, it could elicit symptoms with greater weight (increase in R) or muscle fatigue after a long-distance gait (decrease in E).316171819) In fact, several researchers have recently reported that patients with pes planovalgus could have a variety of symptoms due to the reduction of energy efficiency caused by kinetic loss during exercise including gait.716) In many clinical cases, youths with pes planovalgus complain of abnormal discomfort or pain in the foot-ankle complex, lower leg, or knee joint. Such clinical symptoms include instability of the foot-ankle joint complex, sprains, plantar fasciitis, Achilles tendinitis, and patellofemoral joint pain.316171819) Thus, evaluation of functional loss due to kinetic energy loss would be equally important to morphological indicators in the assessment of patients with pes planovalgus. Nonetheless, there have been few studies on the biomechanical evaluation of pes planovalgus using gait analysis.
Moment is determined (torque [moment] = force × moment arm [d] = force × lever arm [L] × cosθ) in accordance with the amount of operated force, length of lever, and angle at which force was exerted. When the value of θ is 0° (cos0 = 1), as in a normal foot, moment has the maximum value. One reason why pes planovalgus is kinetically disadvantageous is that θ deviates from 0° and ultimately shortens the lever arm compared with the normal foot. This result is caused by pes planovalgus deformity that includes forefoot abduction in the transverse plane, hindfoot valgus in the coronal plane, and midfoot breakage in the sagittal plane.42021)
In children with the symptoms of pes planovalgus in this study, the forefoot was largely abducted (θ value in the transverse plane) compared with the control group, as the average foot AP talonavicular angle was 28.1°. The amount of heel valgus (θ value in the coronal plane) in the patient group was 17° during the stance phase (Fig. 3D), indicating that the valgus deviation of the heel (the θ value) shortened the lever length in the coronal plane. This finding reflects hindfoot valgus, a characteristic feature of pes planovalgus deformity that shortens the length of the lever in the coronal plane.
The second reason why pes planovalgus is kinetically disadvantageous is that the lever becomes more flexible due to the midfoot breakage of the medial longitudinal arch in the sagittal plane. The foot provides a flexible board that can be stably adapted to the ground during the initial stance phase during gait and is converted to a solid lever during the push-off phase to push off from the ground properly. The energy produced by the muscles can be used efficiently only when the lever (foot) becomes solid during the push-off phase.22)
In the sagittal plane, the Meary's angle (lateral talofirst metatarsal angle) was increased by 12.0° on average, reflecting the degree of static midfoot breakage during the stance phase. The degree of kinetic loss due to the lever becoming flexible during the gait is difficult to measure with gait analysis.41323) The degree of maximum foot dorsiflexion (at the end of the second rocker) for the patient group during gait in this study was approximately 6.5°, with no statistically significant reduction compared to the control group. The maximum degree of plantar flexion (at the end of the third rocker) was significantly reduced (p < 0.05). It was expected that in many of the patients the maximum foot dorsiflexion would be reduced due to the tethering of the Achilles tendon, and the amount of plantar flexion would not be affected by flatfoot deformity. However, the kinematic results were the opposite of this hypothesis.
Gait analysis recognizes the entire foot as a solid rod, unlike the recent gait analysis programs that use multi-segment foot model.41323) In other words, the optical tracking device and software misinterpreted the midfoot breakage during the second push-off phase of the gait as increased foot dorsiflexion in the ankle joint. Thus, the kinematic results showed plantar flexion was reduced to the extent the reduction of dorsiflexion was limited in the ankle joint. Furthermore, an insufficient amount of dorsiflexion is compensated by comparable midfoot breakage. In addition, the fact that the scope of overall plantar flexion is reduced during the third rocker represents a decrease in acceleration.
Among children with pes planovalgus in this study, hindfoot valgus and forefoot abduction (talonavicular angle) both increased. Thus, the energy required for supination and inversion to make the foot a solid lever during gait should have been greater. The center line of pressure load during the mid-stance phase is biased outwardly in pes planovalgus, thereby making it difficult for a dynamic pronation–supination transition and reducing the driving force at the end of the stance phase by the abducted–supinated forefoot.
The third reason why pes planovalgus is kinetically disadvantageous is that the reduced Achilles tendon extension cannot generate normal acceleration during push-off. In a study on the joint segmental model, Saraswat et al.24) pointed out that the ankle joint would undergo relative plantar flexion and extroversion since the pitch of the calcaneus in pes planovalgus was shortened and became valgus from a kinematic perspective. The overall ankle joint motion range would also be shortened since the ankle joint would be in a relative state of planar flexion during gait when accompanied by a tight Achilles tendon. Therefore, when the ankle joint motion range, particularly ankle dorsiflexion, is reduced, motion of the adjacent joints such as the knee joint and foot complex will be increased to compensate, in order for the lower leg to move forward from the rear of the ankle joint to the front in the midstance phase. In the knee joint, the plantar flexion-knee extension couple will be increased; therefore, the knee joint will be hyperextended.22) In the foot, the midfoot, which is normally fixed during midstance, becomes mobile, thereby causing midfoot collapse upon weight loading (midfoot breakage of flexible flatfoot). On the contrary, to increase ankle joint dorsiflexion by another compensatory mechanism, it is also possible to walk while slightly bending the knee joint to reduce gastrocnemius tension. The pes planovalgus patient group in this study did not show an increased plantar flexion-knee extension couple. Instead, it demonstrated a gait style that would bend the knee joint slightly with midfoot breakage. But the compensation mechanism might be different according to the gait speed.
When the overall ankle joint motion range and foot lever arm rigidity are reduced, plantar flexion moment is reduced, joint angular velocity is reduced, and ultimately the power of the ankle joint will be decreased. As the Achilles tendon is not appropriately stretched during growth in children with severe pes planovalgus deformity, Achilles tendon lengthening is affected, which is believed to cause a shortening of the Achilles tendon.
In this study, the calcaneus pitch angle of the symptomatic flatfoot group was reduced (11.6° on average) compared with the normal group. The Meary's angle was increased (12.0° on average). These observations indicate that the hindfoot is relatively plantar flexed, and the midfoot has more mobility during stance phase.
Consequently, in this study, the ankle joint moment (0.89 Nm/kg vs. 1.27 Nm/kg) and power (1.38 Nm/kg vs. 2.52 Nm/kg) were significantly lower for the patient group at the last part of the second rocker. Ultimately, pes planovalgus is a complex, multi-joint, multi-plane deformity involving an unfavorable leverage system. To compensate for this insufficient biomechanical skeletal structure, subsidiary abnormal muscle activity might occur, which can cause various muscle fatigue symptoms around foot-ankle complexes.
This study has some limitations. Young adults whose mean age was 21.3 years were selected as the control group, while children with pes planovalgus had a mean age of 9.5 years. For the kinetic study, it was challenging to constitute an age-matched group with normal rigid arched feet. Nonetheless, this study can still be helpful in determining effective and accurate therapeutic methods by conducting an evaluation of kinetic severity using gait analysis in addition to the diagnosis of pes planovalgus using existing methods such as X-ray and footprint.
In conclusion, this study measured the degree of kinetic loss during gait among patients with pes planovalgus by comparing gait analysis data with unaffected controls. From a kinetic perspective, patients with severe pes planovalgus were found to have an approximately 30% loss of moment and 45% loss of power compared to individuals with feet preserving medical longitudinal arches.




 XML Download
XML Download