

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The degeneration of lumbar back muscle is important in the lumbar spine for many reasons. Chronic low back pain has been known to be associated with high fat content of multifidus as one of the back muscle groups.1) Patients with lumbar degenerative kyphosis are also known to be more related with back muscle degeneration than patients with chronic low back pain.2,3) The quality of life was even related to back muscle strength especially in middle ages.4) So, a study about lumbar back muscle degeneration is clinically significant. Besides, the lumbar sagittal profile is another critical topic to predict the clinical outcome in back muscle degeneration. There have been many studies to cover the relationship between a sagittal imbalance of the spine and functional or radiological outcomes. It was published that the lumbar sagittal balance was related to the postoperative recovery rate.5)
In fact, a lumbar degenerative kyphosis is known to be a disease which shows both sagittal imbalance and lumbar back muscle degeneration. However, to the best of our knowledge, the definite relationship between a degeneration of the lumbar back muscle and lumbar sagittal profiles has not been studied yet. The degree of lumbar back muscle degeneration can be measured by modifying the method for fatty muscle degeneration in rotator cuff diseases.6) Spino-pelvic parameters can be obtained from lumbar standing lateral radiographs. It was meaningful to find predictive factors from simple radiographs because the degeneration of lumbar back muscles could not be assessed by simple radiographs. In addition, the authors thought that the gender difference should be considered because muscle mass and strength were different by gender.7) Furthermore, the back muscle fiber size and type distribution is known to be different between male and female.8) The purpose of this study was to search for clinical and radiological factors to predict the degree of lumbar back muscle degeneration by the different gender groups.
METHODS
Materials
This study was a retrospective case series and was approved by Institutional Review Board of Kangwon National University Hostpital.
We reviewed 112 consecutive patients (44 men and 68 women) with lumbar spinal stenosis that underwent one or more level of posterior decompression regardless of fusion between 1 January 2009 and 31 December 2011. Only patients older than 55 years were enrolled. Patients with previous back surgery, neuromuscular disease and spondylodiscitis and also patients that could not preoperatively ambulate were excluded. Also patients were excluded if there femoral head could not be seen in lumbar lateral radiographs because the radiologic parameters could not be measured correctly. Demographic data including age, sex, height, weight, and body mass index (BMI) were obtained from chart reviews. The degree of osteoporosis was derived from bone marrow density (BMD) scores as average T-scores from the first lumbar vertebra to the fourth lumbar vertebra using dual energy X-ray absorptiometry (DEXA; Lunar Prodigy, GE Healthcare, Amersham, UK). The T-score of the spine was dropped from the calculation process if the specific lumbar spine was severely sclerotic due to degenerative changes.
Lumbar spine lateral radiographs were obtained in standing position with arms straightened ahead. The lumbar spine magnetic resonance imaging (MRI) was preoperatively obtained with a 1.5T scanner (Intera Achieva, Philips, Amsterdam, The Netherlands). A sagittal sequence was obtained with T1-weighted spin echo (TR 374.93 ms, TE 11.00 ms) and T2-weighted spin echo (TR 3,500 ms, TE 120 ms). A transverse sequence was obtained by almost the same sequence with an adjustment parallel to the disc level. Four slices with 4 mm thickness at each disc level were obtained with 138 mm × 200 mm field of view.
Methods
The degree of lumbar back muscle degeneration was inferred by the degree of fatty infiltration (FI) with T1 axial section of MRI on a L3-4 disc level. This was classified into 3 categories by the degree of fat signal in muscle layer qualitatively including both multifidus and longissimus: grade 1 (mild) for FI below 10%, grade 2 (moderate) for FI between 10% to 50%, and grade 3 (severe) for FI above 50%.9) Each representative case was illustrated in Fig. 1.
Lumbar lordosis (LL), sacral slope (SS), pelvic tilt (PT), and pelvic incidence (PI) were calculated with lumbar spine standing lateral radiographs using the angle tools in a picture archiving communication system (PACS). The measurements of each parameter were described as an illustration in Fig. 2. The degree of spinal stenosis was classified into 4 grades by the method of Schizas et al.10) The degree of facet arthropathy was also classified into 4 grades by the method of Fujiwara et al.11) The above mentioned two variables were obtained from the axial image of the most severely compressed level and degenerated level, respectively, in MRI. The degrees of FI, spinal stenosis, and facet arthropathy were graded by two spine surgeons independently. Agreement methods were used between them if disparity existed.
Student t-test, chi-square test, or Fisher exact test were used according to the character of variables to compare clinical and radiological parameters between male and female. The analysis of variance (ANOVA) was used to search for a relationship between the degree of lumbar back muscle degeneration and possible related factors in each gender group. All variables significant at a level of less than 0.2 were considered in the linear regression analysis. The p-value less than 0.05 was considered significant in the multivariate model. Each statistical analysis was done using SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Patient Characteristics and Difference between Male and Female
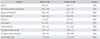
The average age was 68.0 years (male, 68.36 years; female, 68.43 years) and there was no difference between each gender group (p = 0.963). The BMD score, BMI, PI, PT, LL, and the degree of back muscle degeneration showed differences between male and women. The results are summarized in Table 1.
Predictive Factors for Lumbar Back Muscle Degeneration in the Male Group
The age, BMD, PT, SS, and facet arthropathy were adopted as possible related factors with lumbar back muscle degeneration in the univariate analysis. However, only PT showed statistical significance in the linear regression analysis (p = 0.018). The degree of PT, which was increased to an average of 15.3 in grade 1, 20.3 in grade 2, and 24.1 in grade 3, correlated with FI. Age, BMD, SS, and facet arthropathy were not related with the lumbar back muscle degeneration in adjusted model. Results are summarized in Table 2.
Predictive Factors for Lumbar Back Muscle Degeneration in the Female Group
Age, BMI, and PT were adopted as possible related factors with lumbar back muscle degeneration in the univariate analysis. All three variables showed statistical significance in the linear regression model and showed a tendency to increase as the grade of FI was increased. p-values were 0.013, 0.001, and 0.019, respectively. Results are summarized in Table 3.
DISCUSSION
Our results showed PT as the only factor related with lumbar back muscle degeneration in both, the male and female group. Age and BMI were related factors in the female group only. The degree of spinal stenosis and facet joint arthropathy were thought to be possible related factors but did not show any correlation with lumbar back muscle degeneration.
In fact, many studies about the degeneration of the lumbar back muscle have covered both, the volume of back muscle and degree of FI. The cross-sectional area by computed tomography (CT) or MRI has been used in case of back muscle volume measurements. The relationship between the cross-sectional area of back muscles and chronic low back pain, postoperative cross-sectional area changes and the reliability of a checking method for the cross-sectional area have been searched in many studies.12,13,14,15,16) However, studies about the relationship between the degree of FI and other factors including lumbar sagittal profiles were relatively rare. The FI of back muscles are known to be related with chronic low back pain in a few studies.1,17) Also, the FI degrees were compared between groups with degenerative kyphosis group an control groups in previous studies.2,3) In those studies, the degree of back muscle atrophy was more severe in the lumbar degenerative kyphosis group than in the chronic low back pain group. However, to the best of our knowledge, factors to predict the degree of lumbar back muscle degeneration have never been searched before. The authors thought that different factors would be related with back muscle degeneration according to different gender because many clinical and radiological factors were different between them. Those considerations were supported by the current study. It was also supported by an anatomical study about muscle fiber sizes and type differences between genders.8) Therefore, our current study is meaningful too.
The results in our current study were in some aspects concordant with other studies. For instance, a significant association was found between the decrease of paraspinal muscle density and the increase of age and BMI in one study.18) However, gender difference and sagittal profiles were not considered in that study. In fact, the process of muscle degeneration according to aging is naturally intrinsic and a positive trend was found in the male group also (p = 0.103). However, the BMI was not at all related with back muscle degeneration in the male group (p = 0.796). It means, overweight could be an important prognostic factor for lumbar back muscle degeneration in the women group only because the body weight is proportional to the BMI. In fact, there have been controversial results about the relationship between BMI and lumbar back muscle degeneration until now. Although studies suggesting a positive correlation between them exist, many studies have questioned the relationship between BMI and back muscle degeneration or low back pain.18,19,20,21)
Spino-pelvic parameters were other possible factors that may be related with back muscle degeneration. In our study, PT was the only related factor to back muscle degeneration regardless of gender difference. The PT showed an increasing tendency as the back muscle degeneration progressed. In fact, there are not so many researches existing about the relationship between PI, PT, SS, and LL with back muscle degeneration as expected. PT was considered to be important for the surgical outcome of degenerative flat back in one study.22) However, this study focused on indications of surgery for degenerative flat back according to PT. The degree of PT was increased as the pelvic retroversion progressed after lumbar fusion surgery with inadequate LL in another study.23) However, the degree of back muscle degeneration was not directly mentioned in this study as well.
Our study has several limitations. Firstly, the sample size was relatively small, especially in the male group. If there had been more male patients, a more reliable outcome could have been obtained. Secondly, the qualitative design for diagnostic methods to check the lumbar back muscle degeneration was also a limitation. There have been several reports using the quantitative methods with specific software.3,24) However, such studies had its limitations also. Those methods are technically complex, so they are hard to apply to a real clinical situation. In addition, they are prone to leading variable results if the threshold gray-scale value would be differently set. The proportions of fat signal in back muscles were sensitively changed by the threshold gray-scale value in the axial sections of MRI. Thirdly, although our result showed that few different factors were related to lumbar back muscle degeneration according to the different gender, the cause and effect relationship could not be concluded between each factor and muscle degeneration. Lastly, some important factors were not included in this analysis, such as exercising habits or professional employment.
However, the authors think the current study contains of some helpful messages. Based on our study, the degree of lumbar back muscle degeneration which was known to be the possible cause of lumbar degenerative kyphosis and chronic low back pain could be to some degree inferred from a few clinical and radiological factors. It could be helpful for the clinician to predict the degree of back muscle degeneration in out-patient clinics without CT or MRI. In addition, further demographic factors should be considered to predict the back muscle status in case of female patients.
In conclusion, the PT was the important predictive factor for lumbar back muscle degeneration in both, in male and female. However, age and BMI were predictive factors in female patients only. Regardless of gender, other spino-pelvic parameters and MRI findings were not associated with lumbar back muscle degeneration. However, further researches will be needed to verify those predictive factors and to reveal the cause and effect relationship.




 XML Download
XML Download