

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Tenosynovial giant cell tumors, also known as pigmented villonodular tenosynovitis, arise in the synovial tissue of the joint, tendon sheath, mucosal bursa and fibrous tissue adjacent to the tendon.1) These tumors predominantly involve the palmar side of fingers and toes, and seldomly larger joints like the knees and ankles.2) Tenosynovial giant cell tumors of the tendon sheath are rarely intra-articular. There has been only one reported case of tenosynovial giant cell tumor arising from the anterior cruciate ligament (ACL).3) In this case report, we present a rare location of a tenosynovial giant cell tumor arising from femoral attachment of the ACL and its treatment with arthroscopy.
CASE REPORT
A 29-year-old man presented with eight-year history of vague pain in the right knee that aggravated when squatting. He was a sedentary worker. He stated that there had been no prior trauma to the knee. There was no catching, swelling or sense of giving way. On physical examination, there were negative findings on the Lachman and pivot-shift tests and no swelling or tenderness along the joint line. The range of motion was full, with no loss of extension, but painful in extreme range of flexion. Patellar movements were normal and negative on patellar compression test. The findings on radiographs of the knee were interpreted as normal. Magnetic resonance imaging revealed that meniscus and posterior cruciate ligament were normal. Coronal and sagittal T1-weighted images demonstrated that the soft tissue mass was isointense to muscle and obscured the ACL. T2-weighted sagittal magnetic resonance images showed heterogenous, intermediate to low signal intensity, which was slightly higher than that of skeletal muscle (Fig. 1). There were no palpable mass-like lesions on his whole body and no family history of hyperlipidemia or xanthomatosis. Laboratory examinations, including platelet count, prothrombin time, bleeding time and total cholesterol, were all within normal limits. Other blood parameters showed normal range. Arthroscopic examination showed normal findings of both meniscus, posterior cruciate ligament and articular cartilage.
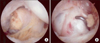
The ACL appeared to be diffusely bulging, but maintained normal tension. Posteromedial and posterolateral portals were made to visualize the mass more clearly. We were able to access the lesions by switching the posterolateral and posteromedial portal alternatively. The mass was located behind the ACL, close to the femoral attachment site. It was round in shape, measuring about 20 mm × 11 mm in diameter with a reddish-brown color (Fig. 2A). It was excised using a motorized instrument and basket forceps by piecemeal (Fig. 2B). A repeat performance of the Lachman test and pivot-shift test showed a stable knee.
Microscopic features varied on different parts of the tumor. The basic cellular composition of the tumor was well-defined polygonal mononuclear cells with a scanty, faintly eosinophilic cytoplasm. In some areas, there were bands or sheets of amorphous collagen (Fig. 3A). Foci of xanthoma cells with foamy cytoplasm and vacuoles were present, accompanied by branching capillaries. Multinucleated giant cells had abundant eosinophilic cytoplasm and contained eight or more nuclei (Fig. 3B). The patient had no further complaints following the operation, and there was no recurrence on 55-months of follow-up.
DISCUSSION
The many synonyms of tenosynovial giant cell tumor reflect its clinicopathologic heterogeneity and historical differences. The various terms used to describe the tumor are: giant cell tumor of tendon sheath, nodular tenosynovitis, pigmented villonodular synovitis, fibroxanthoma and fibrous histiocytoma.4) The four clinicopathologic variants of tenosynovial giant cell tumor are localized, diffuse extra-articular, diffuse intra-articular (diffuse pigmented villonodular synovitis), and malignant.1,5) The localized type of tenosynovial giant cell tumor is defined as a circumscribed lesion that is microscopically not infiltrating into the fat or skeletal muscle. The tumor most commonly occurs in the fingers and may be extra-articular, intra-articular or both.5) Less common is its occurrence in hands and wrists, toes, feet, ankles, knees and rarely in the hip. This tumor is usually diagnosed in young to middle-aged adults between the ages of twenty to fifty, with a female predominance. The tumor typically presents as a slowly growing, painless mass of size between 0.5 to 4.0 cm. Lesions of the knee are usually intra-articular and may cause pain and joint effusion. Following local excision, the digital tumors have some tendency to recur at 10%-20%, but the intra-articular tumors in the knee joint recur with a greater frequency.6) We have found in the literature only one case of localized tenosynovial giant cell tumor that arose from the ACL of the knee.3)
In this case report, we described a histopathologically proven giant cell tumor of the tendon sheath arising from the ACL, which was diagnosed by magnetic resonance imaging. The tumor was totally resected arthroscopically. The patient had no further complaints following the operation, and there was no recurrence at 55-months of long-term follow-up.


 XML Download
XML Download