

 PDF
PDF ePub
ePub Citation
Citation Print
Print


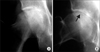
Osteonecrosis (ON) of the femoral head is well known cause of femoral head collapse. When a collapse is observed on radiographs, the diagnosis has generally been considered ON. Recently, subchondral insufficiency fracture (SIF) of the femoral head without any evidence of predisposing ON has been proposed as a new concept regarding femoral head collapse.1,2) SIF also results in femoral head collapse on radiographs; however, it has a totally different pathophysiology from ON (Fig. 1). Histopathologically, SIF has been reported in 5% to 10% of patients who underwent hip replacement with a diagnosis of ON of the femoral head.1) SIF and ON need to be differentiated in terms of precise diagnosis and appropriate treatment.
WHAT IS AN INSUFFICIENCY FRACTURE?
A bone fracture generally occurs due to excessive external force, while a stress fracture occurs when much lower forces are repetitively loaded over a long period of time. Stress fractures are further divided into fatigue fractures, insufficiency fractures, and pathological fractures depending on intrinsic properties (bone characteristics).3)
A fatigue fracture occurs when abnormal stress is applied to bone with normal elastic resistance. In contrast, an insufficiency fracture is produced by normal or physiological stress applied to bone with deficient elastic resistance. Vertebral body fractures secondary to osteoporosis are one of the most common examples of insufficiency fractures. When an insufficiency fracture is observed immediately below the cartilage of a joint, it is called a subchondral insufficiency fracture. The term of pathological fracture is used for any fracture in bone weakened by tumor.3)
SIF OF THE FEMORAL HEAD
Concept
The concept of SIF, first proposed in 1996,4) involves bone fragility usually secondary to osteoporosis or osteopenia leading to subchondral fractures in the femoral head without any evidence of ON.
Hip fractures are an increasingly important public health problem in the elderly. In the United States, it has been estimated that more than 500,000 cases will occur each year by 2030.5) The most common fractures occur in the femoral neck (either subcapital, intertrochanteric or subtrochanteric). Subchondral fractures are most commonly observed as a secondary phenomenon in cases with ON, but there are some case reports of primary subchondral stress fractures in the femoral head in young military trainees.6)
Epidemiology
According to the English literature published between 1996 and 2002, approximately 30 cases of SIF were reported in 3 men and 27 women aged 59-88 years (mean, 72 years). SIF was most commonly observed in elderly women with osteoporosis. Although the precise prevalence of SIF is unknown, recent histopathological re-evaluation has revealed that SIF was observed in 6.3% (460 out of 7,349) patients with a preoperative diagnosis of osteoarthritis, and in 11.1% (41 out of 369) patients with ON.1)
Etiology
Bone fragility due to osteoporosis is considered the most important cause of SIF, similar to vertebral body fractures. The reason why bone fractures occur in the subchondral area is unknown; however, it may be due to the stress applied immediately below the subchondral area. SIF has also been reported in renal7,8) and liver9) transplant recipients, systemic lupus erythematosus patients10) and younger adults.11)
Clinical Symptoms
SIFs of the femoral head typically present with an acute onset of hip pain, occurring as a result of minor injury, such as hip joint twisting, bending forward, or long walks with heavy bags. However, some cases have no such contributing factors. The range of motion, particularly flexion and internal rotation, is limited by pain. In some cases, pain disappears in a few months after onset, but in other cases the pain gradually worsens.
Plain Radiograph Findings
In general, no apparent abnormalities are observed immediately after the onset of pain, except for a decrease in bone density (Fig. 2). In patients without further fracture progression, sclerotic changes due to callus formation are observed in the subchondral area several months later. In patients who progress to collapse, the fracture line is seen as a crescent sign or an irregularly shaped deformity of the femoral head a few weeks after onset (Figs. 1-3). Even when no apparent evidence of fracture is seen on anteroposterior view, it can be observed on the lateral view (the Lauenstein position). Therefore, it is necessary to obtain both views on radiographs.
MRI Findings
Plain radiographs often show no apparent abnormalities in the early phase, so magnetic resonance imaging (MRI) should be performed immediately when SIF is suspected. One of the most characteristic MRI findings is a diffuse bone marrow edema pattern as well as a band-like low signal intensity lesion within the bone marrow edema pattern on T1-weighted imaging (Figs. 2 and 3).1,2,12,13) This band lesion is the most distinctive finding and is essential for the diagnosis of SIF, which histopathologically corresponds to a fracture line with associated repair tissue.13) In addition, the shape of this low intensity band, usually irregular, serpiginous, parallel to the articular surface, and often discontinuous, is useful for the diagnosis (Fig. 4).13) On T2 or gadolinium enhanced images, both the low intensity band and the area between the band and the articular surface tend to show high signal intensity, especially in the early phases of the fracture (Fig. 5).13)
Other Imaging Findings
Bone scintigraphy generally shows diffuse increased uptake throughout the femoral head (Fig. 5).
Prognosis
The prognosis of SIF depends on a number of variables including age, degree of osteopenia, activity, body weight, and extent of fracture, as well as initial treatment. Some cases of SIF have been reported to heal after conservative therapy, including rest, non-weight-bearing, and traction,4,12,14) while other cases have been reported to undergo collapse necessitating surgery.1,2) In addition, some cases show rapid progression of the collapse, such as seen in rapidly progressive arthrosis of the hip (Fig. 3).15,16) The precise prognosis is still unknown.
A recent report on prognostic factors based on MRI findings indicated that the length of the band lesion, corresponding to the length of the fracture line, and the ratio of the band length to the weight bearing portion of the femoral head are important predictive factors.17)
Treatment
In the early phase when no apparent femoral head collapse is observed, conservative therapy, such as rest, non-weight-bearing, use of crutches, and traction, should be attempted. However, when a collapse progresses and pain increases, surgical treatment may be necessary.
Recently, SIF in younger adults aged 20-30 years has been reported.11) Since their fractures are likely to occur in the antero-superior portion of the femoral head, transtrochanteric rotational osteotomy is indicated, and excellent outcomes have been reported.18) In contrast, total hip arthroplasty or hemiarthroplasty is indicated in elderly patients (Fig. 5).
Pathology
Before the pathological concept of SIF was first introduced in 2000,19) the majority of SIF cases would have been diagnosed histologically as ON, presumably based on small foci of necrosis caused by the fracture.1,2) However, such necrotic regions will be observed only around the fracture line and there will be no evidence of antecedent bone infarction or its zonal pattern.19,20)
Histopathological criteria for the diagnosis of subchondral fractures have been established.1,2,19) On gross examination, a linear, narrow, irregular whitish grey zone in the bone marrow space parallel to the subchondral bone endplate is generally seen. Microscopically, this area consists of irregularly arranged fracture callus, reactive cartilage, and granulation tissue (Fig. 2). It should be noted that since all fractures lead to some bone and bone marrow necrosis on either side of the fracture line, small segments of necrotic bone trabeculae may be observed. However, such necrotic regions should not be diagnosed as primary ON.1,19,20) In addition, localized microfractures often observed in the superficial subarticular bone seen in osteoarthritis should not be considered as SIF. In osteoarthritis, fractured bone trabeculae are generally thick, while those in SIF are thin and sparse.21)
DIFFERENTIATION FROM ON OF THE FEMORAL HEAD
The characteristic MRI finding in SIF is a low intensity band on T1 with associated bone marrow edema; however, similar low intensity bands have also been seen in ON.22) Radiographic differentiation between ON and insufficiency fractures appears to be somewhat confusing, but both the clinical picture and MRI characteristics are considered to be useful for the differentiation between ON and SIF (Table 1).
Clinical Findings
SIF is generally seen in elderly women with osteoporosis, who are occasionally obese. Bilateral involvement is rare.1,2,4,12) On the other hand, ON is generally seen in middle-aged patients, often with a history of corticosteroids intake or alcohol abuse. Bilateral involvement is commonly seen in around 50-70%.23) SIF should be suspected in osteoporotic elderly women without any history of corticosteroid use or alcohol abuse.24)
Plain Radiographs
The radiographic appearance of SIF and ON may be similar. In SIF, initial radiographs are often unremarkable or show only mild osteoarthritic changes. Similarly, early ON also shows no or minimal changes. In the advanced stage, a crescent sign is commonly seen in both SIF and ON; therefore, it cannot be used to differentiate between these two conditions (Fig. 1). In addition, the band-like sclerosis in the femoral head, which is characteristic of ON, is also sometimes seen in SIF a few months after onset.
MRI
Several reports have proposed that the shape of the low intensity band on T1 may be useful for differentiating SIF from ON.12,13,24) In SIF, the low intensity band has been reported to have an irregular serpentine shape, often parallel to the articular surface, since it corresponds to a fracture line (Fig. 4).1,2,12,13) On the other hand, the low intensity band in ON often appears as a smooth mirror image of the articular surface, representing the band of repair tissue formed around the wedge-shaped osteonecrotic area (Fig. 4).20,22) However, some cases of SIF have been reported to show a smooth well delineated shape similar to those seen in ON.25) In addition, fractures often occur in the subchondral region in ON, so a serpentine appearance of the low intensity line on T1 can also be seen in ON.26) We should keep in mind that the shape of the low intensity band is not always diagnostic.
A more reliable indicator of SIF is the homogeneously high signal intensity of the proximal segment divided by the fracture line on T2 or gadolinium enhanced images. This corresponds to a proximal segment that is generally alive and consists of repair tissue in SIF. On the other hand, in ON, the subchondral bone segment proximal to the low intensity band does not show a high signal intensity, since the proximal segment is totally necrotic.13) However, when the necrotic region has undergone repair by granulation tissue and appositional bone formation, the proximal segment may show a high signal intensity, even in ON (Fig. 5).27)






 XML Download
XML Download