

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Tension-type headache is the most frequent primary headache disorder in the general population.1,2 The International Headache Society has classified this type of headache into episodic and chronic forms.3 The 1-year prevalence rates of episodic tension-type headache and chronic type are about 38.3% and 2.2%, respectively.4 Chronic tension-type headache is one of the most neglected headache disorders and is difficult to treat.5 It causes substantial levels of disability, not only to patients and their families but also to society.6 It has long been debated whether the pain in chronic tension-type headache originates from myofascial tissues or from central mechanisms in the brain.7
The role of psychological factors in headaches has long been a focus of investigation. Many investigations have shown that patients with primary headache disorders, especially migraine, exhibit some psychological abnormalities. Numerous studies have examined the personality structure of patients with primary headache disorders, and it has been found that such patients were mildly anxious and depressed relative to their headache-free counterparts.8-11 However, there are fewer descriptions in the literature of personality traits in patients with chronic tension-type headache. Patients with chronic tension-type headache have generally experienced more adverse events and rated them as more stressful than did headache-free volunteers.12 A high level of anxiety, neuroticism, or depression has also been found in patients with this headache type.10 Perozzo et al.13 have shown that these patients present a significant impairment of anger control, a higher level of anxiety, depression, phobias and obsessive-compulsive symptoms, emotional lability, and psychophysiological disorders, thus suggesting a connection between anger and the duration of headache experience. Bag et al.14 provided further evidence that negative effects (e.g., depression, anxiety, and hostility) were interrelated and were of greater concern among patients with chronic tension-type headache than among those without pain. Other studies using the Cloninger seven-factor model of the Temperament and Character Inventory also documented an elevated Harm Avoidance score among those with chronic tension-type headache.15-17
Even fewer studies have investigated the psychological features of cervicogenic headache. Cervicogenic headache is typically a unilateral head pain that can be provoked by neck movement, awkward head positions, or pressure on tender points in the neck. Most cases of cervicogenic headache are caused by pathology of the upper cervical spine, but the type and exact location of the pathology varies substantially.18 A higher incidence of various symptoms, including fatigability and irritability, has been found in patients with cervicobrachial pain and headache.19
While chronic tension-type headache (a primary headache disorder) and cervicogenic headache (a secondary headache disorder) share similar clinical manifestations (e.g., pain in the occipital-cervical area, tenderness intensity, or comorbidity with anxiety or depression), we hypothesized that their personality traits differ. For instance, the sensation-seeking or impulsivity trait was found to be less pronounced in patients who have experienced spinal cord injury,20 and this might also be the case in patients with cervicogenic headache.
The five-factor personality model has been the most reproducible method of trait assessment,21,22 and the Zukerman-Kuhlman Personality Questionnaire (ZKPQ)23 is one example of the models used to measure impulsive sensation seeking, and neuroticism-anxiety, aggression-hostility, activity, and sociability. In addition, the Zuckerman Sensation-Seeking Scale (SSS)24 was designed specifically to measure in detail the deviant sensation-seeking trait. Therefore, in this study we administered the ZKPQ and SSS questionnaires to patients with either chronic tension-type headache or cervicogenic headache. Depression is often found to be correlated with personality traits,25,26 we thus also measured the depressive tendency of our participants by administering the Plutchik-van-Praag Depression Inventory (PVP).27 The PVP is interchangeable with other well-known inventories such as the Beck Depression Inventory, the Zung Depression Scale, the Center for Epidemiologic Studies-Depression Questionnaire, and the Minnesota Multiphasic Personality Inventory Depression Scale. It has also been shown to be valid in the Chinese culture and been used in other studies.28,29
Men are more physically active than women,30 and they experience more neck traumas, which results in a male predilection toward cervicogenic headache.31 Indeed, in recent years the traditional gender role differentiation in Chinese society has meant that the psychological stressors in the workplace are experienced more by men than by women.32 We therefore focused on the personality variations of male patients with either cervicogenic or chronic tension-type headache.
Methods
Participants
Sixty-three Chinese men (Han ethnicity) were included in this study, comprising 19 patients with cervicogenic headache, 18 patients with chronic tension-type headache, and 26 healthy volunteers. The headache types were diagnosed according to International Headache Society criteria;3 those with cervicogenic headache were further confirmed 3 months later when the head pain had resolved following successful treatment. The healthy volunteers (age, 35.0±12.4 years, mean±SD; range, 18-67 years) were recruited from the same urban area as the 39 headache patients, and served as controls. None of the healthy participants had experienced headache or other functionally or organically neurological disorders during for the last 3 years. In addition, all of the participants had not consumed alcohol or drugs for at least 72 hours prior to the test and provided written informed consent to participate. Our study design was approved by the Ethics Committee of Zhejiang University School of Medicine. The respective ethical guidelines were followed throughout the study.
Questionnaires
Participants were asked to complete three questionnaires on-site in a quiet room. Each questionnaire is briefly introduced below.
ZKPQ
This questionnaire comprises 99 true/false items, whereby 1 point is awarded for each chosen item corresponding to a personality trait. It measures the following major scales: Impulsive Sensation Seeking (19 items), Neuroticism-Anxiety (19 items), Aggression-Hostility (17 items), Activity (17 items), and Sociability (17 items). Ten items of a lie or infrequency scale were randomly inserted as a validity indicator.20 Any score above 3 on the infrequency scale suggests either inattention to the content of the items and acquiescence or a very strong social desirability set. This questionnaire has been shown to be reliable for use in the Chinese culture.33,34
SSS
The SSS questionnaire was slightly modified by Carton et al.35 (form V, 40 items). One point is awarded for each chosen item corresponding to sensation seeking. This form contains ten items covering the following four scales: Disinhibition, Thrill and Adventure Seeking, Experience Seeking, and Boredom Susceptibility. There is no overlap between the subscale items. The total score in this form is the sum of the four subscale scores. The scales have been shown to be reliable for use in the Chinese culture.36
PVP
Each item of the 34-item PVP is scored 0, 1, or 2, corresponding to increasing depressive tendencies. Participants have "possible depression" if they score between 20 and 25, or "depression" if they score above 25.27
Statistics
Data are expressed as mean±SD values, and were analyzed with SPSS software, version 16.0 (SPSS, Chicago, IL, USA). The five ZKPQ or SSS scales were treated as repeated measures. Therefore, mean personality scores in these groups were analyzed by a two-way ANOVA [i.e., group (3)×scale score (5)]. Mean PVP scores and the individual personality scores in different groups were subjected to one-way ANOVA [i.e., group (3)×scale score (1)]. Once a main effect was detected, post-hoc Dunnett's test was used to analyze the individual mean scale scores in the three groups. The relationships between the ZKPQ, SSS, and PVP scores and headache frequency, duration, or intensity in patients were assessed using the Spearman rank order correlation test. The headache features, intensities, or the psychiatric/migraine comorbidities in the two patient groups were analyzed by the Chi-square test, and the headache durations (per attack or years since onset) in the two patient groups were analyzed using the independent Student's t-test. Results were considered to be significant at p<0.05.
Results
Neither age [main effect, F(2, 60)=0.1, p>0.05, mean squared error (MSE)=21.8] nor education level [main effect, F(2, 60)=2.3, p>0.05, MSE=2.5] differed significantly between the three groups. Information about the headache features, duration (per attack or years since onset), intensity, and the psychiatric/migraine comorbidity for the two patient groups are given in Table 1.
Two-way ANOVA detected significant differences in ZKPQ scale scores between the participating groups [main effect, F(2, 60)=3.1, p<0.05, MSE=54.6]. Post-hoc Duncan's test showed that the scored for ZKPQ Neuroticism-Anxiety was significantly higher in the chronic tension-type headache group (11.5±4.0) than in both the cervicogenic headache group (8.2±4.0) and the healthy controls (7.8±3.7) (Table 2).
Two-way ANOVA also detected significant differences in SSS scores between the three groups [F(2, 60)=4.1, p<0.05, MSE=64.7]. Post-hoc Duncan's test showed that the total SSS score was significantly lower in the cervicogenic headache group (10.1±3.8) than in both the chronic tension-type headache group (13.7±4.5) and the healthy controls (13.6±4.7). More specifically, the score on the SSS Thrill and Adventure Seeking subscale was significantly lower in the cervicogenic headache group (3.7±2.0) than in the healthy controls (5.7±2.7) (Table 3).
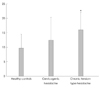
One-way ANOVA detected significant differences in PVP score between the three groups [F(2, 60)=5.6, p<0.05, MSE=38.1]. The PVP scores were significantly higher in the chronic tension-type headache group (16.0±6.0) than in the healthy controls (9.7±4.8) (Fig. 1).
We did not find any correlation between ZKPQ, SSS, and PVP scores and headache frequency and intensity in either the cervicogenic headache or chronic tension-type headache group, or indeed when the data of all patients were pooled. Nor did we find any correlation between duration of headache (per attack or years since onset) and the scale scores in the same patient groups.
Discussion
The aim of the present study was to elucidate the personality traits in chronic tension-type headache and cervicogenic headache using a five-factor personality model (ZKPQ) and a measure for a deviant trait, sensation seeking. We found increased ZKPQ Neuroticism-Anxiety scores in the chronic tension-type headache group and decreased total SSS scores and Thrill and Adventure Seeking subscale scores in the cervicogenic headache group. In addition, depression scores were higher in the chronic tension-type headache group than in the other two groups. The present findings thus concur with most descriptions of personality and mood dysfunctions in sufferers of chronic tension-type headache.10,13,14,37
Individuals with a high Neuroticism-Anxiety score are described as emotionally upset, tense, worried, fearful, obsessively indecisive, lacking in self-confidence, and sensitive to criticism. The chronic tension-type headache group in this study had a high level of neuroticism-anxiety, in accordance with the study of Cao et al.38 who used the same five-factor model. As mentioned previously, high scores for Harm Avoidance have also been found in patients with chronic tension-type headache.15-17 Indeed, the score for Harm Avoidance in Cloninger's Temperament and Character Inventory is significantly correlated with the ZKPQ Neuroticism-Anxiety score.39
Sensation seeking represents the willingness to take risks for the sake of excitement or novel experience. Cervicogenic headache is a secondary head pain that can be provoked by neck movement, awkward head positions, or pressure on tender points in the neck.18 There is a restriction of the motion range in the neck for patients with cervicogenic headache,40 which may lead to a decreased will/ability to move. Consequently, patients with cervicogenic headache display a lower sensation-seeking tendency. This was confined to the Thrill and Adventure Seeking subscale, which implies that patients with this type of headache have less desire to engage in sports or other physical activities involving speed or danger. On the other hand, cervicogenic headache is a heterogenic entity, and a firm clinical diagnostic paradigm that most clinicians can use with confidence is still lacking.41 Ours finding might at least provide personologic evidence to address the pathology of this headache type.
Whether abnormal traits are the causes or consequences of chronic tension-type headache remains to be established. Schoenen suggested that depression is the villain in tension-type headache, rather than just being a bystander.42 Depression can be a factor for tension-type headache, and both depression and anxiety are related to the intensity and frequency of the pain experience.43 In accordance with the literature, we found high neuroticism-anxiety scores and depression in those with chronic tension-type headache, but not in those with cervicogenic headache. On the other hand, we would like to speculate that the lower sensation-seeking scores, and especially those for thrill and adventure seeking found in the cervicogenic headache, are simply a consequence of the activity reduction after the neck trauma.
This study was subject to some limitations. Firstly, although our study design reached an adequate statistical power, the number of participants in each group was small. Our findings in the cervicogenic group in particular need to be confirmed by other independent laboratories worldwide, since this headache population is heterogenic. Secondly, we only included male participants; whether our findings can be generalized to female participants remains to be determined. Thirdly, we did not measure the treatment-seeking tendency of our patients, and it is not known whether this tendency influenced the personality characteristics of our patients.
From a clinical perspective, our findings might encourage the adoption of psychotherapies for these patients, for instance to deliver skills to train those with chronic tension-type headache in emotional control, and in behavioral modification (to elevate the sensation seeking level) for those with cervicogenic headache. The consideration would be particularly the case once a certain personality disorder is comorbid with these headaches.



 XML Download
XML Download