

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Thymoma is reportedly found in 10-30% of patients with myasthenia gravis (MG).1-3 The presence of thymoma is thought to adversely influence the patient's prognosis and to play an important role in the pathophysiology of MG. The ability to accurately identify thymoma will help clinicians and patients to understand the natural history and course of MG. Several previous studies have determined the incidence of thymoma in MG, but the estimates vary widely across studies because of differences in study populations and diagnostic criteria. For example, most study populations were recruited from surgery-based settings, and this is not representative of all MG patients. More accurate estimates of the incidence of thymoma in MG will help inform both patients and their physicians, facilitate health policy discussions, provide etiologic clues, and optimize the management of MG. We conducted a quantitative systematic review of the incidence of thymoma in an observational study of unselected MG patients.
Methods
This systematic review was conducted according to Meta-analysis of Observational Studies in Epidemiology guidelines.4 We collected published studies available from the biomedical literature by searching MEDLINE for relevant articles published between 1960 and January 2012, and Embase for relevant articles published between 1980 and January 2012. Only papers published in English were considered. The key search terms used were "thymoma", "complications", and "myasthenia gravis". Additional studies were located by searching the references lists of the retrieved articles and manually searching the main neurology journals. When several articles were published by the same authors or groups, the publication with the largest sample was selected. We used Cohen's kappa statistic (κ) to assess the level of agreement between the two reviewers.
This review included all incidence studies and case series of unselected MG patients that included information on thymoma. Two types of hospital-based studies were eligible: 1) those with consecutive patient recruitment and 2) those without consecutive patient recruitment but with unselected recruitment (e.g., reviews of all MG patients from a hospital register between defined time-limited boundaries). We excluded studies that conformed with any of the following criteria: 1) limited to specific patient characteristics, such as generalized MG only or late-age MG; 2) limited to MG thymoma but not thymomatous MG; 3) used convenience sampling; and 4) the total sample was less than 20 patients.
Data extraction
Two reviewers extracted information from the articles regarding study design, population characteristics, diagnostic criteria, and thymoma classification. If disagreement persisted after studying the complete manuscript, a third reviewer was consulted. We hypothesized that any heterogeneity might be explained by differences in study designs, with lower incidences expected in population-based studies (which include patients with minor signs or symptoms of neuropathy but are capable of manual work) than in studies where recruitment was restricted to surgery departments. Studies were grouped into three categories according to the degree of case selection, as follows:5,6 1) "population-based studies", which were considered to be of the highest quality (lowest bias); 2) "hospital-based studies", in which patients were enrolled from neurology and surgery departments using unselected hospital enrollment or records; and 3) "surgery-based studies". Although thymus histopathology is regarded as the gold standard in the diagnosis of thymoma, it is anticipated that studies where a diagnosis was made only after thymectomy may result in biases in included patients. In addition, the population-based studies in which thymoma was diagnosed only using the postoperative history method (but not multiple methods of ascertainment, such as computed tomography, or anti-striated-muscle antibody test) were considered as surgery-based studies, and were thus classified into the surgery-based group.
Statistical analysis
Analysis was conducted using Meta-DiSc version 1.4.7 The DerSimonian and Laird (random-effects) method was selected when there was evidence of statistical heterogeneity. The 95% confidence intervals (CIs) of the pooled risk estimates were calculated to allow for extrabinomial variation, because standard methods of calculating 95% CIs produce artificially narrow intervals if there is heterogeneity of risk across the different studies. The heterogeneity of incidence estimates across studies was tested using χ2 tests. The robustness of pooled proportions was explored by conducting sensitivity analyses. Sources of clinical and statistical heterogeneity were explored by means of subgroup and metaregression analyses. The incidence of thymoma was analyzed by regional group (Americas, Europe, and Asia; one study from New Zealand was not analyzed) and calendar year for four periods (1960s, 1980s, 1990s, 2000s; no reports published in the 1970s were identified). We performed additional analyses to identify the factors associated with thymoma in MG by pooling odds ratios (ORs). Specifically, we chose to study factors related to demographic and clinical variables as follows:8 sex (male/female), age at onset of MG (<40 years/≥40 years), Myasthenia Gravis Foundation of America clinical classification, and anti-acetylcholine-receptor antibody test results (seropositive/seronegative). Fixed-effects analysis was used unless there was evidence of heterogeneity (P≤0.1), in which case random-effects analysis was used. Heterogeneity was quantified using I2 values.
Population-based, surgery-based, and hospital-based studies were combined for the calculation of the pooled ORs.5 Where measurement methods for a given variable differed between studies, data were dichotomized as follows: MG onset at <40 years and ≥40 years, and ocular and generalized MG.
Results
Search results
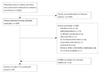
Our search, which was performed on January 2, 2012, identified 2206 articles (Fig. 1). Of these, 1859 were excluded on the basis of their titles or abstracts and 347 reports were identified for full-text review. Eight additional reports were identified by searching relevant reference lists or by hand searches of the main neurology journals. Ultimately, 49 studies fulfilled the inclusion and exclusion criteria and were included in this review.2,3,9-55 The agreement between reviewers for inclusion of articles was almost perfect, at 98.0% (κ=0.92; 95% CI, 0.86-0.97).56
Study characteristics
Table 1 lists the demographic details, study design, and methods used to diagnose thymoma in all of the studies that were relevant to each source of recruitment: population-based (6 studies),3,10,19,31,43,46 hospital-based (4 studies),2,13,25,47 and surgery-based studies (39 studies).9,11,12,14-18,20-24,26-30,32-42,44,45,48-55 All of the studies included patients with standard clinical criteria for MG. No solely prospective studies were included (one study combined prospective and retrospective approaches).51 Two25,47 and ten21,23,26,33,34,37,40,44,45,50 studies used consecutive enrollment in hospital- and surgery-based subgroups, respectively. Various methods were used to diagnose thymoma. Four population-based studies completed thymoma assessment using chest radiography, computed tomography, magnetic resonance imaging, anti-striated-muscle antibody testing, thymic history, autopsy, and biopsy alone or in combination,3,31,43,46 while two population-based studies did not investigate the method of thymoma assessment.10,19 Similar thymoma assessments were used in hospital-based studies. All surgery-based studies confirmed the diagnosis by thymus histopathology. We further classified thymoma diagnosis in surgery-based studies: eight studies15,22,35-37,40,48,54 used the Masaoka Staging System,57 and two studies48,50 used the World Health Organization (WHO) histopathologic classification,58 while other studies differentiated thymomas from other thymic pathologies (e.g., normal thymus and hyperplastic thymus) and did not provide further information.
Incidence of thymoma
The I2 statistic ranged from 64.3% to 84.1% in each subgroup, indicating heterogeneity across the included studies. We therefore used a random-effects model to pool the data. Although the reported incidence of thymoma in MG varied markedly across individual studies, the pooled estimate of all three categories indicated that the incidence of thymoma was 21% (95% CI, 20-22%) in MG patients. The pooled estimated incidences were 17% (95% CI, 14-20%), 12% (95% CI, 11-13%), and 25% (95% CI, 24-26%) in population-, hospital-, and surgery-based studies, respectively (Fig. 2). We hypothesized that selection of population-based case-control studies or cohort studies is important for an accurate estimation. However, the population-based studies were not designed to report on the incidence of thymoma. When analyzed according to regional group, the incidence was 13% (95% CI, 12-15%) for the Americas, 23% (95% CI, 22-24%) for European cases, and 29% (95% CI, 26-31%) for Asian cases. During the four time periods, the incidences were higher in the 1990s (22%; 95% CI, 20-24%) and 2000s (24%; 95% CI, 23-25%) than in the 1960s (17%; 95% CI, 13-22%) and 1980s (16%; 95% CI, 15-18%).
Sensitivity analyses were conducted to explore the robustness of these observations. After removing those studies in which the thymoma diagnosis criteria were not specified and studies published before 1985, the recalculated pooled incidence in each subgroup was similar to the primary pooled results (data not shown). In addition, consecutive/nonconsecutive recruitment was commonly used in case series (e.g., hospital- and surgery-based studies in this review); a separate sensitivity analysis was conducted by removing those studies that did not implement consecutive enrollment. The recalculated pooled incidence [17% (49/288); range, 13-22%] was higher than the overall pooled incidence in hospital-based studies [12% (317/2687); range, 11-13%; p=0.015]. However, the recalculated pooled incidence [22% (213/963); range, 20-25%] was lower than the overall pooled incidence in surgery-based studies [25% (2020/8175); range, 24-26%; p=0.040]. Finally, we performed metaregression analyses of the impact of sample size, publication year, and the diagnostic criteria used on the incidence estimates. No apparent relationships were found between these variables.
We further described the incidence of thymoma in MG using Masaoka's thymoma classification system (I, II, III, and IV). The WHO system was not adopted in this case due to its limited use in the included studies. As a consequence, we extracted these data using invasive/noninvasive thymoma status (where I equals a noninvasive status, and II, III, and IV equal an invasive status). Finally, most of the thymomas in these MG patients were noninvasive (p<0.001).
Data on the clinical association between the incidence of thymoma in MG were available from 5 population-based studies,3,10,19,31,43 1 hospital-based study,13 and 13 surgery-based studies (Table 2).11,15,17,21,22,30,37,41,44,50,51,53,54 Pooled analysis showed that the incidence of thymoma was significantly higher among male MG patients (OR, 1.78; p<0.0001) and those aged ≥40 years at MG onset (OR, 5.74; p<0.00001). None of the selected studies reported the results of anti-acetylcholine-receptor testing focusing on patients with or without thymoma.
Discussion
This was a systematic review of published studies on thymoma in MG. The results of this study suggest that 1) approximately 21% of MG patients develop thymoma, 2) the incidence of thymomatous MG is significantly higher among those who were ≥40 years at MG onset and male MG patients, and 3) the most frequently occurring thymoma in thymomatous-MG patients is the noninvasive type. However, we recognize that there are likely to be some limitations to the interpretation of these estimates. First, there is the potential for underreporting (or underrecognition) of thymoma in population- and hospital-based studies. This may have contributed to the difficulties inherent in the identification of thymoma and hyperplasia in some patients, and particularly in those who did not undergo thymectomy or autopsy and in whom diagnosis was based on the patient's history. Second, the incidence of thymoma in the surgery-based group may have been overestimated due to sampling biases. Furthermore, the generally poor quality of studies also contributes to the limitations of the present study.
Heterogeneity across study estimates remains an important factor limiting the interpretation of our results. Although we attempted to minimize heterogeneity in this review by grouping studies according to the source of case selection, the I2 statistic ranged from 64% to 84%, indicating a high degree of heterogeneity in each group. There are several possible reasons for this. First, multiple methods were often used to diagnose thymoma, with some studies failing to use a validated reference standard to identify thymoma (e.g., a small thymoma is difficult to prove on chest radiography). Second, methods such as computed tomography scans or immunohistochemistry with anti-striated-muscle antibodies all have inherent limitations when used to diagnose thymoma. For example, nearly 20% patients are not detected using anti-striated-muscle antibodies.59,60 Furthermore, although it is well known that thymic histopathology is the gold standard for diagnosis, thymectomy usually tends to be performed in those patients with thymoma or a more severe status, and this would result in selection bias. Therefore, it is not surprising to find that the incidence of thymoma appears to be overestimated in surgery-department-based studies.
It should be noted that all studies included in this review used retrospective recruitment methods. Since retrospective studies are more prone to selection bias, it is difficult to determine whether the heterogeneity in the study estimates represents true differences in the characteristics of populations, biases in the reference standards used, or other errors.
Of course, heterogeneity across studies can also be attributed to differences in case mix, including variation in MG features, clinical characteristics, and sample size. In addition, the thymoma incidence appears to vary between regions. Specifically, the incidence was higher among Asians and lower in the Americas. These differences highlight the possible role of genetic factors (e.g., human leukocyte antigen) in thymoma pathogenesis.61 However, when interpreting our results it should be remembered that the incidence of thymoma in the Americas in this review was greatly influenced by the study of Papatestas et al.,13 which had a very large sample (2062 patients), and in which the incidence of thymoma was only 11%. As there was a lack of detailed descriptions of the type of thymoma assessment used in that study, these findings should be interpreted with caution.
A trend toward an increase in the incidence of thymoma in MG was observed over the four decades analyzed. The lower incidences reported in earlier years (i.e., before 1990) were also likely to have been influenced by the study of Papatestas et al.,13 which was published in 1987, although possible improvements in clinical diagnosis may also have contributed to the apparent increases in the identification of thymoma over those four decades. We attempted to evaluate the characteristics of the populations studied (spectrum of ages and Myasthenia Gravis Foundation of America clinical classification) and thymoma status (classification by WHO or Masaoka), but most of the study reports did not provide this information. This should be taken as a reminder to the MG community of the need to improve the uniformity of methods used to evaluate thymoma, thus enabling a better identification of risk classification or prognostic factors.58,62
Risk analyses suggested that MG patients aged ≥40 years and male MG patients have a higher risk of thymoma in MG. Differences in immunological background, such as a tendency toward a higher incidence of titin and ryanodine receptor antibodies in elderly-onset MG may partly explain this feature.63 Moreover, males have a higher risk than females for tumors at many sites, which might be due to a higher prevalence of occupational or other environmental exposures in males. Together this information leads to possible directions of future pathological studies. One unexpected finding from this review was that noninvasive thymoma occurs more frequently than invasive thymoma among MG patients. This suggests that the symptoms of MG prompt the early detection of thymoma. Another important observation from this systematic review is that although the sample sizes varied markedly across the studies (varying from 21 to 2479 patients), the samples were generally limited (ranging from 33-142) (Table 1) in population-based studies in which thymoma assessment was completed. Thus, there is an urgent need for a well-planned population-based study with a sufficient sample size and including a complete assessment of thymoma in included MG patients.
Strengths and weaknesses of this review
By synthesising all of the published data on thymomas, we have provided a more precise estimate of its incidence in MG than was previously available. The influence of variation in study designs was diluted by pooling all of the available data, and we were able to explore this heterogeneity by examining study characteristics and conducting subgroup analyses. This review was subject to some limitations. First, some of the studies were not originally designed to determine the incidence of thymoma, and were thus more likely to use a nonstandard reference for the assessment of thymoma, resulting in incomplete case ascertainment (e.g., MG patients who have minor signs or symptoms may not have been willing to submit to evaluation for thymoma). Hence, the incidence of thymoma could have been underestimated among these cases. Second, the calculation of the pooled incidence did not include data from all studies in our review because the data were not always provided in a format that enabled pooling. This limits the precision of our results. Furthermore, our study does not provide information on global thymic status. For example, although the thymic pathology exhibited hyperplasia in 80-90% of the MG patients, the evaluation of thymic hyperplasia was not possible in our study. Finally, like most meta-analytic reviews, we pooled studies that exhibited significant heterogeneity.5,7
Conclusion
We have provided some evidence for the incidence of thymoma from three different types of MG studies. Well-planned population-based and prospective cohort studies on the incidence of thymoma in MG are needed to expand our understanding of this association, despite the acknowledged difficulties in analyzing the outcome of chronic and rare diseases with unpredictable and fluctuating courses. A proper diagnostic assessment and uniform evaluation should be applied to participating MG patients.



 XML Download
XML Download