

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Neurocutaneous melanosis (NCM) is a rare congenital, noninheritable neurocutaneous syndrome, characterized by the presence of large and/or multiple congenital melanocytic nevi (CMN) associated with melanosis or melanoma that usually appear in the leptomeninges. Although the clinical presentations of NCM vary with age, NCM is generally accompanied by significant neurological deficits. However, NCM as a cause of epilepsy without any neurological deficit is extremely rare. We report a case of chronic partial epilepsy caused by pathologically proven parenchymal NCM in the brain without leptomeningeal involvement, that was successfully treated surgically.
Case Report
A 32-year-old right-handed man visited our epilepsy clinic due to drug-resistant partial epilepsy. His seizures started at the age of 22 years, since when he had suffered from frequent episodes of disgusting odor and light-headedness despite antiepileptic drug treatment. Also, he had occasionally experienced motionless staring followed by generalized tonic-clonic seizures when he had not complied with treatment. His familial and own medical histories were not remarkable, and the findings of a neurological examination were normal. Electroencephalography (EEG) showed frequent right temporal sharp waves with maximal negativity in the ipsilateral nasopharyngeal electrode. Brain MRI showed a small focal lesion in the lateral part of the right amygdala. The lesion was hyperintense on a T2-weighted image and hypointense on a T1-weighted image without gadolinium enhancement (Fig. 1), which suggested a benign tumor.1 There were multiple large black pigmented nevi on the back, scalp, and posterior neck area, which had existed from birth. The largest black nevus was on his back, covering 9% of his body surface area (1.82 m2).
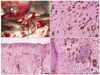
The right temporal lobe including the amygdaloid lesion was excised. Intraoperative electrocorticography before resection revealed active spikes around the lesion. The amygdala lesion was a grayish-to-black friable soft tissue without definite mass formation. There was no meningeal melanosis. The pathology investigation of the lesion demonstrated numerous melanophages. The skin biopsy of the scalp lesion showed that it was an intradermal nevus, as expected (Fig. 2). He was seizure-free (including aura) during the 15-month postsurgery follow-up period.
Discussion
Kadonaga and Frieden2 proposed the following criteria in 1991 that are currently used to diagnose NCM: 1) large and/or multiple CMN in association with meningeal melanosis or melanoma; 2) no evidence of cutaneous melanoma, except in patients with histologically benign meningeal lesions; and 3) no evidence of meningeal melanoma, except in patients with histologically benign cutaneous lesions. The second and third definitions exclude the possibility of metastases from the skin to the central nervous system (CNS) and vice versa, respectively.
CMN are classified into large, medium, and small nevi according to their size:3 larger than 20 cm in an adult, 1.5 to 19.9 cm, and smaller than 1.5 cm, respectively. The term "multiple" is used when more than three lesions are present. Kadonaga and Freiden2 found that 66% of NCM patients had large nevi, and the remaining 34% had numerous pigmented lesions in the absence of a single large congenital melanocytic nevus. In their study, all NCM patients had either posterior midline nevi or head and neck lesions, which suggests that the posterior axial distribution is an important risk factor for developing NCM. Our patient also had multiple medium-sized CMN with a posterior axial distribution.
Embryologically, melanocytes originate from the neural crest and migrate to various sites in the body, such as the basal layer of the epidermis, pia mater, leptomeninges, medullary reticular formation, and substantia nigra of the midbrain.4 It is thought that CMN and NCM are caused by the arrest or aberrancy of this normal developmental pattern. In NCM, pigmented thickening of the leptomeninges is most frequent in areas with melanocytes.4 Parenchymal melanosis is less common than leptomeningeal melanosis, and caused by primary involvement of the melanin-containing macrophages and melanocytes, or secondary spread via Virchow-Robin spaces from the leptomeninges. The pathology investigation of our patient showed melanin-containing macrophages, and revealed parenchymal melanosis without leptomeningeal melanosis.
The neurological manifestations of NCM vary with age.2 Before the age of 2 years, the most common initial clinical signs and symptoms of NCM are related to increased intracranial pressure, including headache (35%), vomiting (42%), generalized seizures (48%), increased head circumference (23%), cranial nerve palsies (26%; in particular VI), papilledema (10%), and meningeal signs (3%).6 The subset of patients with a discrete intracranial mass becomes symptomatic when older (mean age, 12.8 years; range, from birth to 65 years) and is more likely to develop focal seizures, localized sensorimotor deficits, difficulties with speech, or psychiatric symptoms.6 Our patient became symptomatic with partial seizures when he was 22 years old.
The prognosis of symptomatic NCM is poor. Most of the 33 NCM patients in a study involving giant CMN7 demonstrated the first neurologic symptom when they were younger than 5 years. Eighty-two percent of the patients died by the time of reporting, and the median age at death was 3 years. However, most of the patients had diffuse leptomeningeal involvement or melanoma. While symptomatic NCM is estimated to occur in less than 3% of patients with giant CMN,7 one study found MRI evidence of CNS melanosis in 10 (23%) of 42 asymptomatic giant-CMN patients,8 among whom only 1 had subsequently developed symptomatic disease during an average follow-up of 5 years. Because the MRI findings of these 10 patients showed parenchymal NCM without diffuse leptomeningeal involvement, the prognosis of parenchymal NCM appears to be much better than that of typical NCM with diffuse leptomeningeal involvement or melanoma. Our patient with parenchymal melanosis subsequently developed epilepsy without neurological deficits.
Melanin pigment is inherently paramagnetic, and hence melanin deposits in NCM show a high signal intensity on T1-weighted MRI and a low signal intensity on T2-weighted MRI. This pattern of parenchymal melanosis appears to be most evident and frequent at the amygdala and adjacent anterior temporal cortex.8 In our patient, brain MRI showed the typical location but an atypical pattern of hyperintensity on T2-weighted images and isointensity on T1-weighted images.
NCM appears to be a rare cause of chronic partial epilepsy. Some cases with chronic epilepsy related to NCM have been reported, but most of them had other conditions such as CNS melanoma, mental retardation, psychosis, and diffuse leptomeningeal involvement with neurologic deficits.9 To our knowledge, the only surgical case with NCM similar to our patient was a 29-year-old woman with normal psychomotor development and intelligence who had right temporal-lobe epilepsy due to amygdaloid melanosis and underwent right temporal resection.10 Here we have reported a surgically successful case of chronic partial epilepsy caused by pathologically proven parenchymal NCM without leptomeningeal involvement. Therefore, NCM occurring in the brain parenchyma should be considered as a cause of chronic partial epilepsy.

 XML Download
XML Download