

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Snoring is primary symptom and sign of upper airway narrowing during sleep whose severity ranges from benign primary snoring to snoring associated with severe obstructive sleep apnea (OSA).1 Although snoring is common in all age groups, studies have found that its prevalence in adolescents varies widely, which is due to differences in study methods (e.g., self-reported data or sleep-laboratory data), definition of snoring frequency, ethnicity, and who reported the snoring (e.g., the subjects or their parents). Previous studies have involved adolescents aged 12 to 18 years. In a community-based sample of 1,014 adolescent–parent pairs in the Detroit metropolitan area, more than 20% of the adolescents snored at least a few nights per month, and apnea-like symptoms were reported to affect 2.5–6.1% of adolescents aged 13 to 16 years.2 In contrast, in a cross-sectional study (n=1,030) in Turkey, 4.0% of parents reported that their children aged 12 to 17 years habitually snored.3 However, these studies were limited by their inclusion of only a regional population in each country.
It is important to recognize the presence of sleep problems, particularly in adolescents, whose sleep disturbances may considerably affect their daytime functioning and physical and psychological development. In addition, sleep-related breathing disorder (SRBD) is reportedly associated with excessive daytime sleepiness (EDS) and poor school performance.24 To our knowledge, although some regional studies have shown the prevalence of snoring and witnessed apnea in 2,336 students from senior high schools of Gyeonggi province in Korea,5 there has been no nationwide population-based study of the prevalence of self-perceived snoring/apnea in Korean adolescents. The purpose of the present study was therefore to estimate the prevalence of self-perceived snoring/apnea and to determine how these conditions are associated with daytime sleepiness in students from the first grade to the third grade of high school (10–12th grades) in Korea.
METHODS
Subjects
A nationwide cross-sectional study was performed from July 1 to 31, 2011 by the Sleep Center at Samsung Medical Center and the Korea Centers for Disease Control and Prevention on sleep health status and its effect upon daily life in Korean adolescents. We included high-school students in the 15 districts of Korea. The nationwide selection of schools and gathering of information about the students were supported by the Ministry of Education, Science and Technology. In total, 75 high schools (grades 10–12) were randomly selected. Each school had approximately 30 students in each class, and 2 classes were randomly selected in each grade at each school to represent the overall population of that grade. This study was approved by the Institutional Review Board at Samsung Medical Center (Seoul, Korea).
Measures
This study used an online survey. Each student who participated in the survey was asked to complete a questionnaire in the computer room at their school. All students in each class participated at the same time. The students answered the following two questions about self-perceived snoring/apnea occurred in the past 30 days: “How often did you snore loudly in the past 30 days?” and “How often did you hold your breath, have breathing pauses, or stop breathing when sleeping in the past 30 days?” There were four possible answers to each question: never, occasionally, often, or always. To calculate the prevalence of self-perceived snoring/apnea, we included students who answered “occasionally”, “often”, and “always” to the two questions on snoring/apnea. The sleep duration during a school day was obtained by self-reporting. The subjective perception of the sufficiency of sleep duration was evaluated with the question “What is your perceived sleep duration?” The possible answers to this question were adequate, considerable, or insufficient.
All participants completed the Korean version of the Epworth Sleepiness Scale (ESS) by self-assessment. The ESS is an eight-item questionnaire that measures daytime sleepiness; it was translated into Korean, and the Korean version of the ESS was validated.6 Each item is assigned an estimated score from 0 to 3, and the total score is the sum of the scores for the eight items. The last item of the ESS questionnaire was originally designed for a driver (“In a car, while stopped for a few minutes in the traffic”), and so this was modified to a question for a passenger because persons younger than 20 years are not allowed to drive in Korea.7 The total ESS score ranges from 0 to 24, and students with an ESS score of ≥11 were considered to have EDS.
Body mass index (BMI) was calculated from the self-reported weight and height of the students using the standard formula [BMI=weight (kg)/height (m2)] and then categorized into the following four classes according to the 2007 Korean National Growth Charts: underweight (<5th percentile), overweight (85–95th percentile), obese (≥95th percentile or ≥25 kg/m2), and normal.8
Statistical analysis
Logistic regression was performed to estimate adjusted odds ratios (ORs) and 95% confidence intervals (CIs) of self-perceived snoring/apnea after adjusting for sex, school grade, and BMI. The chi-square test was applied to quantify the effects of clinical variables on the prevalence of EDS. We also used logistic regression to examine the OR and 95% CI values of EDS associated with the frequencies of self-perceived snoring (model 1) and apnea (model 2), including adjustment for relevant covariates. The covariates in these two models were sex, school grade, BMI category (underweight, normal, overweight, and obese), sleep duration during a school day (<5, ≥5 and <6, ≥6 and <7, and ≥7 hours/day), and subjective perception of sleep duration (adequate, considerable, and insufficient). Data were analyzed using STATA® (version 11.0, StataCorp., College Station, TX, USA).
RESULTS
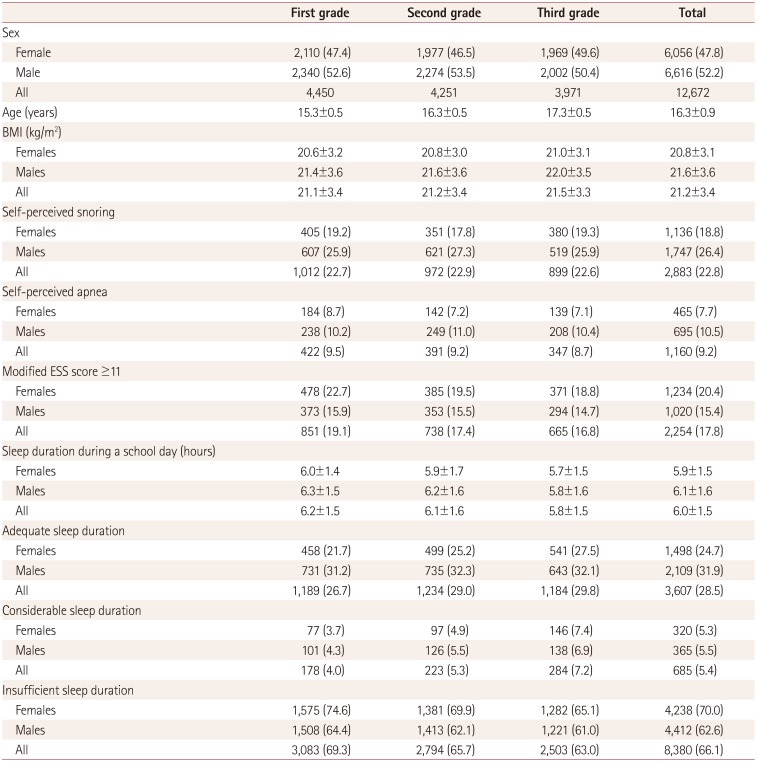
In total, of 12,672 high-school students participated in this study, comprising 6,056 (47.8%) females and 6,616 (52.2%) males. The participants were aged 16.3±0.9 years (mean±SD) and had a BMI of 21.2±3.4 kg/m2. Table 1 lists the demographic and clinical characteristics of the students in each grade. Self-perceived snoring was observed in 2,883 (22.8%) students (18.8% for females and 26.4% for males) occasionally (in 16.5%), often (in 4.2%), and always (in 2.0%). Self-perceived apnea was reported in 1,160 (9.2%) students (7.7% for females and 10.5% for males) occasionally (in 7.2%), often (in 1.4%), and always (0.5%). In total, 2,254 (17.8%) students had a modified ESS score of ≥11. The sleep duration during a school day was 6.0±1.5 hours. The sleep duration was subjectively perceived as being adequate, considerable, and insufficient by 3,607 (28.5%), 685 (5.4%), and 8,380 (66.1%) of the students, respectively.
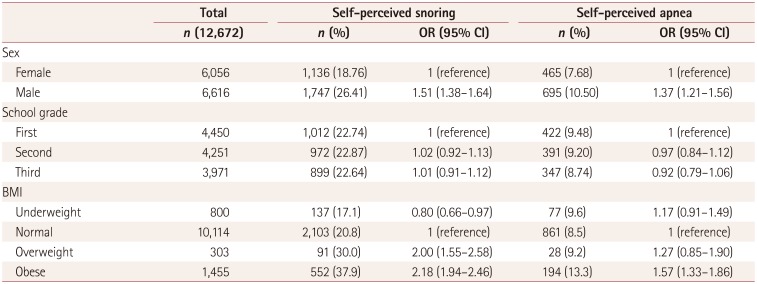
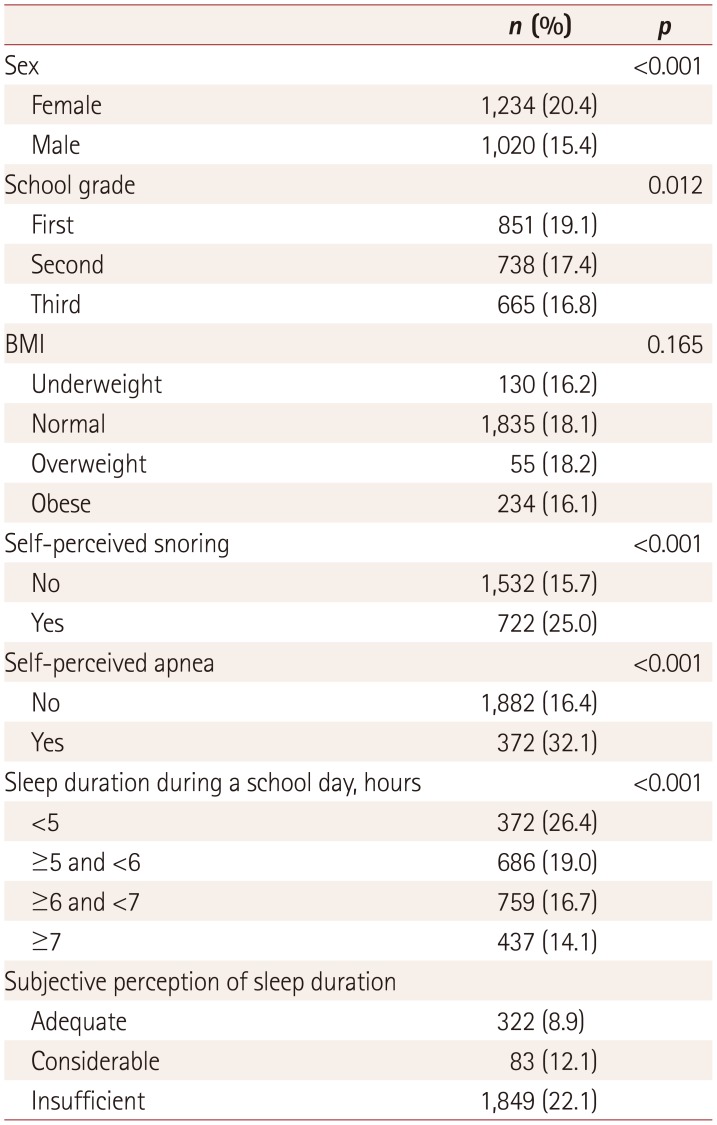
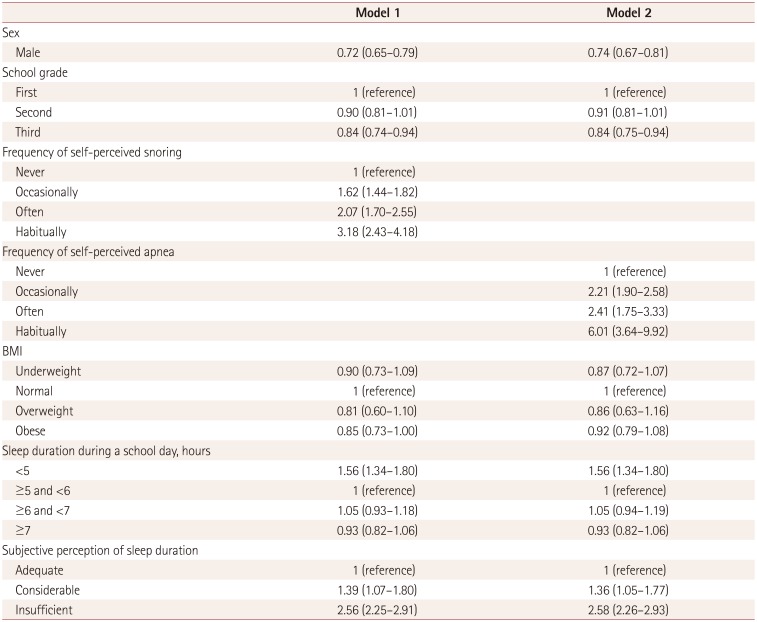
Table 2 lists the prevalence of self-perceived snoring/apnea according to sex, school grade, and BMI. Being male and obese were associated with a higher risk of snoring/apnea. The prevalence of EDS (modified ESS score ≥11) was significantly higher in females (20.4%), first-grade students (19.1%), and students who self-reported that they snored (25.0%) and had apnea (32.1%). The prevalence rates of EDS were 26.4, 19, 16.7, and 14.1% in those with sleep durations of <5, ≥5 and <6, ≥6 and <7, and ≥7 hours, respectively. EDS was reported more frequently in students with an insufficient sleep duration (22.1%) (Table 3). A multivariate analysis found that being female, a first-grade student (vs. third grade), and any frequency of snoring/apnea were associated with EDS. The OR of EDS increased significantly with the frequency of snoring/apnea. A sleep duration of <5 hours during a school day and subjective perceptions of insufficient and considerable sleep durations were significantly associated with EDS, whereas BMI was not associated with EDS in models 1 and 2 (Table 4).
DISCUSSION
In this nationwide sample of first-to third-grade Korean highschool students (i.e., spanning three grades), self-perceived snoring/apnea were observed in 22.8% and 9.2% of the students, respectively. Self-perceived snoring/apnea were significantly more prevalent in males and obese students, and were significantly associated with EDS. The previously reported prevalence of snoring has varied widely with the age and sex of the subjects and the definition of snoring. Two studies of younger children found that 15.8% and 34.6% of those aged 3–11 and 5–13 years, respectively, snore occasionally, while 4.9% and 7% are habitual snorers.910 A study of European adults found that 40.3% reported that they snore regularly, with the prevalence of snoring increasing for ages up to 55 years.11 In addition, 3.8% of the subjects reported breathing pauses while snoring, which were more common in those aged 55–64 years.11 Snoring and breathing pauses have been reported in 23% and 7% of older adults in the United States, respectively.12 The overall prevalence of snoring in the present study of Korean high-school students (aged approximately 15 to 17 years) was lower (16.5% occasionally and 2.0% always) than that in a previous study of a community-based sample of adolescents with student and parent pairs in the Detroit metropolitan area.2 The Detroit study included 1,014 adolescents aged 13 to 16 years, which were younger than our students, and found that more than 20% of the adolescents snored at least a few nights per month, 56.8% did not snore, and 6% snored every or nearly every night (6% reported by parents and 5.8% reported by the adolescents themselves), compared to only 2.0% of the students in the present study “always” snoring.
Johnson and Roth.2 investigated other symptoms associated with SRBD (e.g., awakening with the feeling of gasping or choking), and found that approximately 6.0% of adolescents aged 12–18 years may experience some of these symptoms at least once per week according to independent reports of both students and parents. The prevalence of habitual snoring (often or always) was 4.0% based on parental reports in a study conducted in Turkey.3 Among a sample of subjects aged 13–18 years in Greece, 3.8% habitually snored every night and 0.9% exhibited witnessed apnea episodes every night according to reports of their parents.13 The self-awareness of snoring/apnea is usually lower than that witnessed by family members, especially co-sleepers, and the prevalence varies between self-reported questionnaires and parental reports.
Several studies have defined snoring frequency in different ways. Our study showed that self-perceived snoring reported occurred occasionally, often, and always by 16.5, 4.2, and 2.0%, of the subjects, respectively; the corresponding proportions for self-perceived apnea were 7.2, 1.4, and 0.5%. A study from Spain found that approximately 28 and 14.8% of adolescents aged 12–16 years reportedly snored at least sometimes and often, respectively, and 3% had subjective sleep apnea.14 It should be remembered that there are limitations in comparing snoring/apnea prevalence rates between studies due to country-related social and cultural differences in how their frequencies are defined.
Sex differences in sleep apnea have been reported in general populations. Most epidemiological studies have found the prevalence of sleep apnea to be higher in men than in women, with the male-to-female ratio ranging from approximately 2:1 to 3:1 in adults.151617 However, no sex difference in SRBD symptoms was found among Detroit community-dwelling adolescents aged 13–16 years2 or among Turkish adolescents aged 12–17 years who snored.3 Clinical and polygraphic findings for adolescents aged 12 to 16 years showed that the prevalence of snoring was similar in boys and girls, although this was only for a small sample (n=101).14
The present study found that self-perceived snoring/apnea were more common in males. A previous study of adolescents showed that snoring every night was more common in Greek boys aged 13–18 years than in girls.13 In contrast to adult SRBD, which shows a clear predominance for snoring among men, reported sex differences in SRBD among adolescents have been inconsistent.
The prevalence of SRBD increases with age.18 This present study found that the prevalence of self-perceived snoring and apnea did not vary with grade among Korean high-school students. This result is similar to the Detroit community-based study showing no difference in the prevalence of sleep-disordered breathing symptoms with school grades among subjects aged 13–16 years.2 However, most studies of SRBD in adolescents have included only a narrow age range that may be insufficient for evaluating the effect of age on the prevalence of SRBD in adolescents.
Most epidemiological studies have shown a significant association between OSA and increased body weight in adults. Obesity as a strong factor for OSA is prevalent in Western countries but is less common in Asian countries. Although the degree of the correlation varies with race, BMI is associated with OSA.192021 The association of BMI with SRBD was found to be twice as strong among Caucasian adolescents as among African-American adolescents.2 The waist-to-hip ratio has also been reported to be higher in people who snore.14 We also observed the OR was highest for self-perceived snoring (OR=2.18) and apnea (OR=1.57) in the obese group relative to the normal group.
SRBD is independently associated with EDS: EDS occurs twice as frequently in adolescents with SRBD than in those without SRBD.2 EDS is a major and the most frequently presenting symptom in subjects with OSA.2223 However, EDS does not always occur in patients with OSA. Some studies have found no significant correlation between ESS scores as a subjective evaluation of EDS and apnea-hypopnea indices in polysomnography.242526 However, we found that EDS was associated with the prevalence of self-perceived snoring/apnea. The risk of EDS increased significantly with the frequency of snoring/apnea after adjusting for sex, school grade, BMI, sleep duration during a school day, and subjective perception of sleep duration.
We additionally found that EDS was more common in females, even though self-perceived snoring/apnea was less common than in males. Although sex differences have been found in community-based studies,2728 several studies have produced conflicting findings.2930 This inconsistency may be due to differences in sampling methods between the various studies that led to different sex ratios in the included populations, or in the ESS used to measure daytime sleepiness, since men and women could have answered the surveys differently. Even though we did not evaluate psychophysiological factors such as emotion, menstrual cycle, and daily physical activity, these factors should be considered as possible contributors to sex differences in EDS because they can each differ with sex. Although the third-grade students had subjective sleep insufficiency, they perceived less daytime sleepiness than the first-grade students. The ESS may be a less-sensitive measure of subjective sleepiness in third-grade students–who are college preparatory students–than in first-grade students.
The main limitation of our study relates to the use of a self-reported questionnaire, which is likely to have underestimated the prevalence. However, this study included a large sample of 12,672 students, so it is meaningful in showing a significant association between EDS and snoring/apnea as self-perceived by Korean adolescents. In addition, this was the first nationwide population-based study of the prevalence of self-perceived snoring/apnea in Korean adolescents. We focused on school grade rather than age. Because school hours, physical activities, and academic burden differ between grades, these variables can influence EDS via social factors.
We used both the sleep duration during a school day and the subjective perception of sleep sufficiency as variables for indicating an insufficient sleep duration. The relationship between the sleep duration during a school day and EDS was linear among the included Korean high-school students. Although the relationship was linear, the students with a subjective perception of insufficient or considerable sleep duration had greater EDS than those with an adequate sleep duration. It is possible that subjects suffering from poor sleep quality caused by snoring/apnea and a short sleep duration during a school day are able extend their nocturnal sleep to compensate for EDS. However, the academic burden of high school means that they cannot sleep during a school day, instead sleeping for longer during a no-school day. It is known that EDS is associated with short sleep duration, subjective sleep insufficiency, and unmet sleep duration (sleep need minus the habitual sleep duration) in terms of an insufficient sleep duration. When sleep duration and unmet sleep duration were examined together, only the unmet sleep duration was associated with EDS. Habitual sleep duration was not significantly associated with EDS after adjusting for the unmet sleep duration. EDS was associated with unmet sleep duration, insomnia, high frequency of snoring, and BMI after adjusting for sociodemographic factors in an adult population.31
The sleep habits and school life need to be investigated thoroughly when evaluating the factors influencing EDS in adolescents. We did not investigate various underlying sleep disorders that could be causes of EDS. Moreover, no objective evaluation of sleep duration or quality was available in our data. Our results should therefore be interpreted with caution.
This study found that the prevalence of self-perceived snoring/apnea was significantly higher in males and those who were obese. EDS was more common in students with self-perceived snoring/apnea, and the risk of EDS increased with the frequency of these conditions.
 XML Download
XML Download