

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Restless legs syndrome (RLS) is a common sensorimotor-related sleep disorder, the pathophysiology of which is currently unclear. In addition to the dopamine hypothesis, iron availability in the brain is thought to contribute to RLS.1 There is some evidence from cerebrospinal fluid (CSF),2,3,4 transcranial ultrasonography,5 and autopsy studies to support a connection between brain iron status and RLS, with findings of reduced brain iron content and impaired iron regulation of specific brain lesions in RLS patients.6,7
T2 relaxometry using magnetic resonance imaging (MRI) has been used to measure the iron content in brain regions of patients with various neurological disorders,8,9,10 including RLS.11,12,13,14,15,16 However, the results of previous MRI studies of RLS are conflicting, especially pertaining to the iron content in the substantia nigra (SN) in early- and late-onset RLS patients. Furthermore, the iron index obtained using strong-field MRI (e.g., with a 3.0-tesla magnet) is more sensitive to brain iron levels than that obtained at low field strength.17 Thus, further investigation of this subject is required. Therefore, in the present study the iron contents in the SN and other brain regions were explored in patients with idiopathic RLS (early onset and late onset) and in control subjects using a 3-tesla MRI system. Since the findings of the CSF3,4 and autopsy studies6 support the hypothesis that there is an iron deficit in early-onset RLS, our primary hypothesis was that the SN iron index is lower in early-onset RLS patients than in control subjects.
Methods
Subjects
Thirty-seven patients with idiopathic RLS who were older than 18 years and 40 healthy control subjects were enrolled in this study. All of the patients were diagnosed through a clinical interview by a board-certified Korean neurologist with expertise in RLS diagnosis, using the validated Korean version18 of the Johns Hopkins telephone diagnostic questionnaire.19 Patients with peripheral iron deficiency without definite cause were included, but patients were excluded if they had secondary RLS caused by pregnancy or by other diseases such as chronic kidney disease or peripheral neuropathy, or other sleep disorders such as sleep-disordered breathing, circadian sleep disorders, and parasomnia, as assessed by clinical interview and analysis of sleep questionnaires. These questionnaires included validated Korean versions.20,21,22 The severity of RLS symptoms was evaluated using the validated Korean version23 of the International RLS scale (K-IRLS).24 All RLS subjects had moderateto-severe RLS symptoms (K-IRLS score ≥15). Twenty patients with RLS had early-onset disease, with symptoms starting before 45 years of age, while 17 patients were considered to have late-onset disease. All of the control subjects were free of symptoms indicating RLS, periodic limb movements during sleep (PLMS), or any other sleep disorder. We did not conduct polysomnographic studies, and the presence of PLMS or another sleep disorder was based on the reported history. None of the subjects had any serious medical disorders or brain structural abnormalities on MRI.
All of the RLS patients and 16 control subjects underwent laboratory tests including serum ferritin levels, serum iron levels, and total iron binding capacity on the day of the MRI scan. The MRI was performed during the daytime when patients were asymptomatic. Patients who were already being treated with a dopaminergic agent did not stop their medication for the MRI scan.
All of the subjects gave written informed consent to participate, and the study and its protocol were approved by the institutional review board of a regional hospital.
Imaging protocol
Magnetic Resonance Imaging data were acquired by using a GE VHi scanner operating at 3.0-tesla (GE Medical Systems, Milwaukee, WI, USA). The protocol was as follows:
1) For structural imaging, a T1-weighted, high-resolution, three-dimensional spoiled gradient echo sequence was obtained [repetition time (TR)/echo time (TE)=6 ms/2.2 ms; flip angle=20°; field of view=240 mm; matrix=256×256; 152 axial slices; and slice thickness=2 mm].
2) For T2 relaxometry, a spin echo (SE) sequence was obtained (TR=3725 ms; TE=30, 60, 70, 90, 120, 140, 210, and 280 ms; slice thickness=3 mm; and space=2 mm).
3) For T2* relaxometry, a gradient echo sampling of the free induction decay and echo sequence was obtained (TR=2700 ms; TE=30, 60, 70, 90, 120, and 140 ms; slice thickness=3 mm; and space=2 mm).24
Patients with any structural lesion on T1-weighted, high-resolution, three-dimensional spoiled gradient-echo sequence that could cause secondary RLS were excluded.
Image analysis
T2 and T2* maps were processed using an MRI analysis calculator plug-in in the ImageJ software (http://rsb.info.nih.gov/ij/) created by Karl Schmidt (kfschmidt@bwh.harvard.edu). T2 and T2* maps were produced through a pixel-by-pixel fitting process using the curve fitter class in the ImageJ software. T2 and T2* maps were converted to R2 and R2* maps, respectively, and R2' maps were calculated using an image calculation function in the ImageJ software.
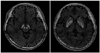
R2, R2*, and R2' maps were obtained following previously described reconstruction procedures.17 The R2' map was used as the 'iron index' because of its higher iron-related specificity. Relaxation rates were measured for five regions: caudate head, putamen, globus pallidus, red nucleus, and SN. Two trained analysts (Y.S.L. and Y.S.Y.) outlined the regions of interest (ROIs) on the SE image using Medical Image Processing, Analysis, and Visualization (MIPAV) software. They were blinded to the status of the subjects and from each other's results. For the SN and red nucleus, the analysts automatically generated the ROIs using MIPAV software, and they were able to manually adjust the border of any ROIs that were broken (semiautomatic method). The ROIs were traced manually for the caudate head, putamen, and globus pallidus (Fig. 1). All of the ROIs were reviewed for accuracy by a neuroradiologist (H.W.C.) independently and blindly. Relaxation rates for ROIs on both the right and left sides were averaged together. The primary ROI was the SN; the secondary ROI measures were the other four brain structures (i.e., caudate head, putamen, globus pallidus, and red nucleus). The intraobserver variability was checked by having one of the researchers (Y.S.L.) perform the same procedure in the SN of all subjects as well as other regions of 14 randomly chosen subjects.
Statistical analysis
The normality of distribution of the parameters was studied using the Kolmogorov-Smirnov test. Analysis of covariance (ANCOVA) was used to compare the age-adjusted iron indexes of the patients and control subjects. Results were assumed to be significant at p<0.05. The correlations between the iron index and disease severity, and the K-IRLS total and subfactors of the K-IRLS (related to symptom severity) were explored using the partial correlation coefficient (with age as a control variable). For our exploratory analyses of four brain regions except SN (early-onset RLS vs. controls, and late-onset RLS vs. controls), we applied ANCOVA with a Bonferroni correction for the eight tests to maintain the overall type 1 error at a level of 0.05. Both intraobserver and interobserver variabilities on relaxation rate measurements were assessed using the Pearson product-moment correlation coefficient.
Results
The clinical characteristics of the study population are in given in Table 1. There were no significant differences in age, gender, and serum ferritin level between the control group and either the early- or late-onset RLS group. The disease duration was significantly longer in the early-onset group than in the late-onset group (p=0.001). The mean K-IRLS score in the de novo state did not differ significantly between the early- and late-onset groups. The percentage of patients with dopaminergic treatment was 35% (7/20) in the early-onset RLS group and 29.4% (5/17) in the late-onset RLS group; the difference was not statistically significant.
The interobserver reliability of the iron index was 0.97, and the intraobserver variability was 0.93 overall. The interobserver and intraobserver variabilities for each brain region exceeded 0.80, with no significant difference, which indicates a strong interobserver and intraobserver agreement. No significant difference was found in the iron index between the anatomic structures of the two hemispheres.
The mean iron index of the SN did not differ significantly between the early-onset group and the control group (p=0.968), but was significantly lower in the late-onset RLS group than in the control group (p=0.034) (Table 2). No significant correlation was found between the SN iron index and the K-IRLS total score, the K-IRLS symptom-severity-related score, the serum ferritin level, the age at symptom onset, or the disease duration for the late-onset RLS group.
Exploratory analyses did not reveal any differences in the iron index between the early-onset RLS group and controls in all other regions. There were no significant differences in any brain region other than the SN between the late-onset RLS group and the controls.
Discussion
This study found a significantly decreased regional iron index in the SN of late-onset RLS patients compared to the controls. However, there was no significant decrease in the SN iron index in the early-onset RLS patients compared to the controls. There was no significant difference in the iron index of any of the other four brain regions between the control and earlyand late-onset RLS patients.
Previous T2 relaxometry studies have variously found decreases or nonsignificant differences in iron content for several brain regions, and especially for the SN (Table 3). A decreased iron content in the SN of early-onset RLS patients was found in early studies,11,12 and similar results were found by an autopsy study.6 However, more recent studies yielded different results. Godau et al.13 found multiregional iron deficiencies in idiopathic RLS, but not in the SN. Astrakas et al.14 reported that late-onset RLS was associated with low iron content in the SN pars compacta. Although we did not evaluate the SN pars compacta and pars reticulata separately, this result is consistent with the present findings. Knake et al.15 did not find any difference in the iron content between idiopathic RLS patients and controls, while Margariti et al.16 found an increase in the iron contents in the subthalamic nucleus and the globus pallidus, but not in the SN of early-onset RLS patients.
These conflicting results regarding the iron content in the SN of idiopathic RLS patients may be due to study heterogeneity. First, although all of the participants in the two early studies11,12 and in the autopsy study6 had been treated with dopaminergic medication, the patients in the larger second study12 were subjected to a drug-free period of at least 7 days. The two more recent studies14,16 included untreated patients only, and the present study included both untreated and treated (about 30%) patients in both groups. Treatment-induced changes in the iron index may account for these differences between the early and more recent studies. It has been shown that treatment with dopamine agonist can affect the release of endogenous dopamine,25 and consequently the amount of dopamine metabolite available. A recent study revealed that the dopamine metabolite aminochrome modified the levels of iron transporters in a way that causes iron accumulation.26 Further investigation is needed to elucidate the treatment-induced changes in the iron content in specific brain regions in RLS patients.
The second possible explanation for the differential findings could be the use of different MRI protocol and image analysis techniques, including the primary measurement (T2 vs. R2') and the methods for ROI evaluation. There is evidence that R2' mapping has a higher iron-related specificity due to the small iron-independent component compared with R2 (1/T2),17,27 and that the use of a strong field (e.g., with a 3.0-tesla magnet) for R2' mapping enables the measurement of small areas such as the SN.28 Therefore, we designed the present study so that the primary measurement was R2' using a 3.0-tesla MRI. In addition, the iron may not be distributed evenly throughout the tissue of a specific ROI, so we tried to include the total area of specific brain regions by using manually adjusted ROIs. Furthermore, we attempted to ensure that the measured iron value was as representative and objective as possible.
In accordance with previous studies,12,14 we found no correlation between the iron index in the SN of late-onset patients and the disease severity. This may be explained by the T2 relaxometry providing information only about the ferritin-bound iron content, and not the total tissue iron, cellular components, or subtypes of ferritin.17 It is expected that the content of bioavailable iron would be correlated with disease severity. Since histopathological studies of the SN in late-onset RLS have not yet been performed, further research is needed.
A limitation to this study was that the data needed to be adjusted using statistical methods due to the age distribution differing between the late-onset RLS patients and the control subjects. In addition, we did not analyze the SN pars compacta and pars reticulata separately, due to the difficulty in drawing the MRI boundary of the SN pars reticulata29 and the low interobserver and intraobserver reliabilities (data not shown).
In summary, the findings of this strong-field (3.0-tesla) T2 relaxometry study demonstrate that late-onset RLS is associated with decreased iron content in the SN, and that the iron content in the SN does not differ significantly between early-onset RLS patients and controls. These findings support the role of regional brain iron deficiency in the pathophysiology of late-onset RLS.



 XML Download
XML Download